
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Research ArticleDOI Number : 10.36811/ijapr.2021.110004Article Views : 1Article Downloads : 1
Psoas hematomas in COVID 19 patients
Hafiani Y*, ELAIASSI M, LAKRAFI A, NSSIRI A, ALHARRAR R, Ezzouine H, Chara B, Mouhaoui M, Aissaoui O, Mounir A, Elkettani C, Baroub L, Benghanem M and Afif MH
Service de réanimation COVID 19 CHU IBN ROCHD Casablanca Morocco
*Corresponding Author: Hafiani Yassine, Service de réanimation COVID 19 CHU IBN ROCHD Casablanca Morocco, Email: alaa-lakrafi@hotmail.fr
Article Information
Aritcle Type: Research Article
Citation: Hafiani Y, Elaiassi M, Lakrafi A, et al. 2021. Psoas hematomas in COVID 19 patients. Int J Anesthesi Pain Res. 3: 01-05.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2021; Hafiani Y
Publication history:
Received date: 04 February, 2021Accepted date: 17 February, 2021
Published date: 18 February, 2021
Abstract
The psoas hematoma Is a frequent complication of anticoagulant treatment and is the first diagnosis to Be made in any patient on anticoagulants with psoitis, the diagnoses Will Be made on the basis of ultrasound or CT examinassions and the treatment Most often consists of 'abstention.
Keywords: Psoas hématome; COVID; Mechanical ventilation; Embolisation; Surgery; Epigastric artery rupture
Introduction
OVID-19 disease is a highly thrombogenic pathology requiring anticoagulation at a curative dose to prevent occurrence of pulmonary embolism or deep thrombosis, in addition to thromboembolic risk it has a component hemorrhagic manifested by bleeding at localizations multiple. Among these hemorrhages, muscle hematomas deep classified as severe bleeding. They are conventionally treated with conservative treatment with the discontinuation of drug and specific reversion, and in rare cases, by surgical evacuation. However, the spread or reappearance of bleeding, although the effect of anticoagulants has been canceled, should suggest additional etiology.
Material and Methods
We conducted a retrospective study extending from July 2020 to December 2020 which allowed us to collect 6 observations of 6different patients. In our study were included patients whom has had a psoas hematoma associated or not with other bleeding. We were looking to determine the frequency and risk factors for the occurrence of psoas hematomas in covid patients in order to isolate a risk profile for developing psoas hematoma during covid and specify the different therapeutic indications. All of our patients have benefited from a daily assessment of NFS-PQ / hemostasis assessment / anti Xa activity. The diagnosis was suspected by clinical signs and confirmed by radiology.
Results
Our study identified 6 cases of psoas hematomas with a sex ratio (m/w) of 2 and an average age of 63 years. 4 of our patients either 67% had comorbidities with type of diabetes and hypertension for only 2 patients without any notable antecedents, 5 out of 6 patients, i.e., 83% were overweight with a BMI greater than 25. 2 of our patients were intubated, ie 33%. 5 out of 6 patients, i.e., 83% received an anti-coagulant treatment based on of LMWH at a dose of 0.8ml times 2 / d and one patient received a dose of 0.6 ml times 2/d. All our patients have benefited from a biological assessment complete with NFS-PQ- hemostasis-anti Xa activity assessment, none of our patients did not present with thrombocytopenia or hemostasis and all of our patients had anti Xa activity in the normal range.2 out of 6 patients were intubated on admission, i.e. 33% of our patients ventilated under controlled mode with FIO2 = 100%, Vt = 380,FR = 20, PEP ranging from 9 to 12cmH2O. 4 patients or 67% of patients benefited from 3 NIV sessions per day with FIO2 = 100%, AI = 12,PEP = 8 cmH2O with alternation between sessions by a MHC at one flow between 12 and 15 L of o2. 1 out of 2 intubated patients was extubated after 10 days of intubation and was reintubated 3 days later for neurological degradation. The circumstances of discovery of the hematoma were variable in 3 patients the hematoma was suspected due to a bruise and swelling of the iliac fossa then confirmed by echo and abdominal CT. In 2 patients the hematoma was discovered on abdominal CT muscle which was motivated by the deglobalization of the patients not improving after transfusion. In one patient it was suspected in front of a picture of hip pain with paresis and paresthesia in the thigh and subsequently confirmed by abdominal CT. All of our patients presented with deglobalization after the occurrence of the hematoma. It was noted that the time between the start of anticoagulant therapy and the onset of the hematoma was on average 5 days with extremes ranging from 2 days to 10 days and the time between intubation and the onset of the hematoma was 4 days. The time between extubation and onset of hematoma was 2 days. We adopted an expectant attitude in all patients with discontinuation of the HBPM and the antiplatelet agent, the course was marked by resorption of the hematoma in 3 of our patients, with the death of one of our patients due to hemodynamic in stability. the evolution in 2 of our patients was marked by worsening hemodynamically rapid, suggesting a surgery but the 2 patients died before performing the gesture.

Abdominal CT scan showing a hematoma of the right psoas measuring 5cm.
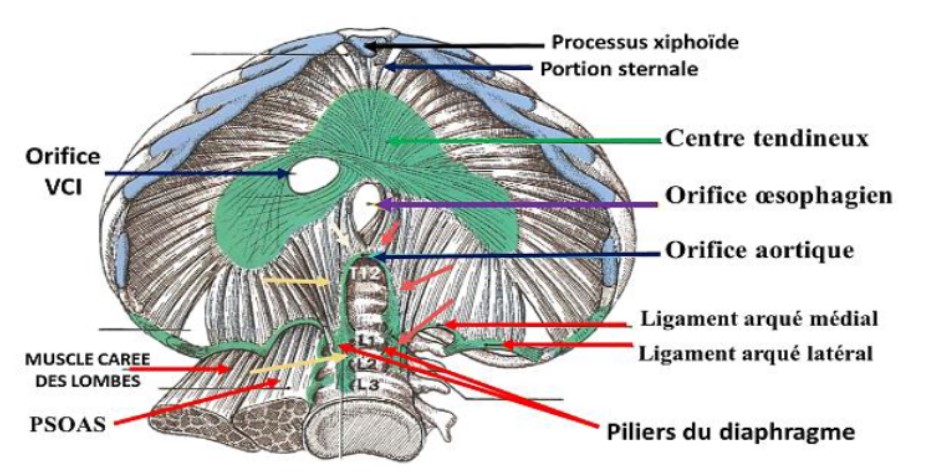
From an anatomical point of view, the ilio-psoas comprises three muscle heads: the psoas major, the psoas muscle minor and the iliac muscle. The bulkier is the muscle psoas major. It arises from the lower half of the D12 vertebra, the first four lumbar vertebrae and the L4-L5 disc and ends on the lesser trochanter after passing through the medial arched ligament of the diaphragm. A muscle small intestine, the psoas minor muscle, is sometimes attached to it. It is ends on the unnamed line. The iliac muscle, originating of the internal iliac fossa, leaves the iliac canal passing behind the psoas major muscle and ends in a tendon common with the latter on the lesser trochanter. Its action is the flexion of the thigh over the pelvis. The termination of muscle on the lesser trochanter communicates the retro peritoneal compartment, where the muscle takes its origins, with the root of the thigh. The relationship of the psoas muscle to the diaphragm thus explains the spread of bleeding following microtraumas of the psoas muscle, due to the effort of coughing towards the pelvis and inguinal orifice.
One of the causes of high mortality in patients with COVID-19 is at an increased risk of clotting disseminated intravascular disease (DIC) and thromboembolism venous, as evidenced by a coagulation profile modified as high D-dimers. It has been proposed that this hypercoagulability phenomenon is due to an increase pro-inflammatory cytokine, mainly IL-6 in patients infected with COVID-19 [1]. These cytokines inflammatory agents facilitate atherosclerotic deposits by local inflammation, plaque rupture and changes hemodynamics. Pro-inflammatory cytokines have also found to be elevated and one of the causes of DIC which can be observed in septic patients. This state hypercoagulability causes thrombi microvascular cells causing failure of several organs and death and should be treated with agents antithrombotic such as heparin [2]. Treatment by anticoagulation at a therapeutic dose may be beneficial but remains controversial. A treatment blood thinners and antiplatelet drugs supplements, such as aspirin, increase the risk of major bleeding complications such as retroperitoneal hemorrhage [3]. The psoas muscle can accumulate up to 10 times its own volume and hematoma of the psoas due to bleeding retroperitoneal may present with hypotension, abdominal pain or low hemoglobin as seen in our patients. Computed tomography remains the initial imaging of choice in case of suspected retroperitoneal bleeding. Initial treatment includes stopping anticoagulants, transfusion therapy, volume resuscitation and supportive measures. The hemodynamically unstable patients on treatment anticoagulant with unpredictable tissue hematomas can be treated by embolization arterial because it is minimally invasive with a rapid therapy compared to surgical treatment. When an active psoas hematoma bleeding is observed, arterial embolization of the third and fourth lumbar arteries is usually justified, this which remains a technical challenge because it requires catheterization selective hemorrhagic artery, embolization and post-embolization studies to document the success of treatment. We currently know that thrombi lungs in COVID-19 develop as a result of vascular damage associated with viral infection and severe inflammation, as evidenced by their levels of D-dimers and inflammatory markers and the increase several thrombolytic factors such as IL-6 and anti-phospholipid antibodies [4]. In this context, high pathophysiological dose heparin may not only be ineffective, but it can also be harmful, possibly contributing to the component hemorrhagic described of microangiopathy. We have certainly need further high-quality studies, preferably randomized trials, to determine whether full dose heparin is warranted, how long it must be continued after discharge of COVID patients- 19 and is it better than the single dose of heparin prophylactic be used to reduce mortality every confused causes. However, we already know that high dose heparin use increases the levels of fatal and major bleeding, that's why this report cases and others raise these concerns because we need better evidence to support this convenient [5]. The genesis of bleeding from the inferior epigastric artery remains mysterious. However, many factors different must be taken into account [6]. First of all, the presence of cough, which is a common symptom of COVID19, which can lead to a significant increase abdominal pressure and, therefore, rupture arterial with subsequent bleeding. In literature het here is a description of intercostal arterial rupture and a rare case of rupture of the gastroduodenal artery after severe cough [7,8]. In our current management of covid the use a high level of PEP in invasive ventilation to ensuring optimal recruitment is likely to induce a abdominal hyper pressure syndrome increasing the risk rupture of the inferior hypogastric artery which could explain the occurrence of a psoas hematoma, for the rest of our patients who have benefited from NIV sessions occurrence of psoas hematoma could be due to mal adjustment to the patient's struggle with the entraining respirator an intra-abdominal hyper pressure syndrome aggravated by cough and inducing a risk of rupture of the epigastric a retrying responsible for the hematoma. Changing from positive chest pressure in mechanical ventilation to negative chest pressure after extubation leads to an increase in intra pressure abdominal worsening by cough which may be responsible of a ruptured lower epigastric artery.
Conclusion
The psoas hematoma is the first diagnosis to be made in a patient on anticoagulant treatment presenting with psoit is associated or not with a sensory-motor deficit, if recurrence of the hematoma after stopping anticoagulants and appropriate treatment it will eliminate coagulopathy congenital then evoke a tumor origin. The treatment is most often abstention and surgery is reserved for cases where there are persistent neurological signs.
References
1. Wada H, Tanigawa M, Wakita Y, et al. 1993. Increased plasma level of interleukin-6 in disseminated intravascular coagulation. Blood Coagula Fibrinolysis. 4: 583-590. Ref.: https://pubmed.ncbi.nlm.nih.gov/8218855/ Doi: https://doi.org/10.1097/00001721-199308000-00009
2. Zhou F, Yu T, Du R, et al. 2020. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. 395: 1054-1062. Ref.: https://pubmed.ncbi.nlm.nih.gov/32171076/ Doi: https://doi.org/10.1016/S0140-6736(20)30566-3
3. Ishan Patel, a Arda Akoluk, a Steven Douedi, a, et al. Flynn Life-Threatening Psoas Hematoma due to Retroperitoneal Hemorrhage in a COVID-19 Patient on Enoxaparin Treated with Arterial Embolization: A Case Report.
4. Papageorgiou C, Jourdi G, Adjambri E, et al. 2018. Disseminated intravascular coagulation: an update on pathogenesis, diagnosis, and therapeutic strategies. 24: 8-28. Ref.: https://pubmed.ncbi.nlm.nih.gov/30296833/ Doi: https://doi.org/10.1177/1076029618806424
5. Klok FA, Kruip M, van der Meer NJM, et al. 2020. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: An updated analysis. 191: 148-150. Ref.: https://pubmed.ncbi.nlm.nih.gov/32381264/ Doi: https://doi.org/10.1016/j.thromres.2020.04.041
6. Amole AO, Kathuria MK, Ozkan OS, et al. 2008. Lumbar artery laceration with retroperitoneal hematoma after placement of a G-2 inferior vena cava filter. Cardiovasc Intervent Radiol. 31: 1257-1259. Ref.: https://pubmed.ncbi.nlm.nih.gov/18543029/ Doi: https://doi.org/10.1007/s00270-008-9365-x
7. Amole AO, Kathuria MK, Ozkan OS, et al. 2008. Lumbar artery laceration with retroperitoneal hematoma after placement of a G-2 inferior vena cava filter. Cardiovasc Intervent Radiol. 31: 1257-1259. Ref.: https://pubmed.ncbi.nlm.nih.gov/18543029/ Doi: https://doi.org/10.1007/s00270-008-9365-x
8. Nik V, Martinek V, Padr R, et al. 2005. Embolization of lumbar artery due to retro peritoneal bleeding following renal biopsy. Nephrol Dial Transplant. 20: 820-822. Ref. : https://pubmed.ncbi.nlm.nih.gov/15772268/ Doi: https://doi.org/10.1093/ndt/gfh685


















