
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Research ArticleDOI Number : 10.36811/ijfs.2019.110003Article Views : 19Article Downloads : 34
A case of fatal intracranial haemorrhage due to ruptured berry aneurysm
Eman Ahmed Alaa El-Din1*, Heba El Sayed Mostafa1, Maha Hasanin Kamel2 and Mohamed Salah Abdelkhalek2
1 Department of Forensic Medicine & Clinical Toxicolcogy, Faculty of Medicine, Zagazig University, Zagazig, Egypt
2Egyptian Forensic Medicine Authority, Cairo, Egypt
*Corresponding author: Eman Ahmed Alaa El-Din, Associate Professor of Forensic Medicine and Toxicology, Departments of Forensic Medicine & Clinical Toxicology, Faculty of Medicine, Zagazig University, Egypt, Tel: +201226026944; Email Eman_alaa77@yahoo.com
Article Information
Aritcle Type: Research Article
Citation: Eman Ahmed Alaa El-Din, Heba El Sayed Mostafa, Maha Hasanin Kamel, et al. 2019. A case of fatal intracranial haemorrhage due to ruptured berry aneurysm. Int J Forensic Sci. 1: 19-26.
Copyright:This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2019; Eman Ahmed Alaa El-Din
Publication history:
Received date: 16 May, 2019Accepted date: 04 June, 2019
Published date: 06 June, 2019
Abstract:
Background: Sudden unexplained deaths in consequence of cerebral causes in adults are a critical section of the medicolegal practice. Berry aneurysms are eminent entities that cause a serious medical condition, like a haemorrhagic stroke, which leads to brain damage and may account for a quarter of cerebrovascular deaths. These aneurysms arise no symptoms for a protracted period or could rupture and bring out intracranial haemorrhage and sudden natural death, thus arousing suspicion.
Aim of the study: This case highlights one of the causes of sudden natural death due to cranial haemorrhage.
Methods: Our case was male 40 years old was found dead on the floor of the bathroom in his home. He has no history of smoking or medical record with an average body built, no risk factors were found. The prosecution report stated that the manner of death was unexplained. The case had undergone full external examination and X-ray for the whole body then medicolegal autopsy. Laboratory investigations were done to show if there was any drug was taken to assist or cause death. We had reviewed the literature concerning the case and attempted to confirm the legal scenario.
Results: On external examination, abrasion was found on the nose and knee. The xray didn’t demonstrate any fractures or foreign body. Urine drug screen revealed negative results for the drug of abuse. The autopsy showed rupture of berry aneurysm at the circle of Willis which and subarachnoid haemorrhage in addition to intraventricular and pontine haemorrhages.
Conclusions: Meticulous examination of such cases could lead to a more precise task of the reason for death, which may have significant implications for surviving family members, and could initiate a better comprehension of the natural history of these intracranial lesions.
Keywords: Aneurysm; Circle of wills; Intracranial haemorrhage; Sudden death; Hypertension.
Introduction
Sudden non-traumatic death is now currently described as natural unexpected death occurring within 1 h of new symptoms. The majority of studies regarding this topic focused on cardiac causes of death because most of the cases are related to cardiovascular disease, especially coronary artery disease [1]. Though, sudden death may have a wide variety of non-cardiac causes, including pulmonary emboli, internal haemorrhage, and sickle cell crises, in addition to a variety of intracranial causes. Moreover, in a few publications, no cause was identified in 12% of cases. Such statistics highlight the significance of a meticulous post-mortem examination in all cases of unexpected death [2-3].Intracranial causes of sudden, non-traumatic death include epilepsy, intraventricular cysts, brain tumours, acute purulent meningitis, hydrocephalus, and ischemic stroke, as Well as rapid bleeding into any one or more of the intracranial compartments: extradural, subdural, subarachnoid, or intraventricular spaces or into the brain parenchyma [4].The causes of intracranial haemorrhage vary depending upon age and anatomical location of the haemorrhage. In most instances, there is bleeding into more than one intracranial compartment. For example, rupture of a berry aneurysm may be associated with a subdural hematoma, bleeding into the subarachnoid space, and an intracerebral hematoma, which in the course of expanding may in turn rupture into the ventricular system [3]. Here, we present a case of sudden and unexpected death due to rupture of a berry aneurysm in an adult male.
Case
A 40-year-old male was found dead on the floor of the bathroom in his home. He has no history of smoking or medical record with an average body built, no risk factors were found. The prosecution report stated that the manner of death was unexplained as he was found lying on the face in the bathroom.
External examination
A medicolegal autopsy was performed. The body was confirmed to be of normal development, with a height of 173 cm. Evidence of blunt trauma was found on the right side of the nose and left knee (Figure 1a,b): Abrasions and subcutaneous haemorrhage were found. These external traumatic signs were assumed to have occurred due to contact with the ground after the decedent fell forward. No injury was found in the occipital region. Post-mortem hypostasis was dark blue in colour. No other abnormities were found during the external examination.

Figure 1: External examination showing: abrasion and subcutaneous haemorrhage were found on: A- the right side of the nose & B- the left knee.
Autopsy examination
Head: There was no evidence of scalp trauma or fracture inside or outside the skull. Gross examination of the brain showed diffuse bilateral basilar subarachnoid haemorrhage (Figure 2), intraventricular haemorrhage (Figure 3a,b), Pontine and cerebellar haemorrhage (Figure 2). Cross-sectioning of the brain revealed a massive intracerebral haemorrhage, with profuse blood filling the cerebral ventricles. The brainstem, cerebellum, showed massive haemorrhage (Figure 6a,b). Other gross autopsy findings included mild to moderate atherosclerosis involving the circle of Willis and multiple atheromatous plaques (Whitish in colour) could be detected (Figure 3). Also, ruptured berry aneurysm of the circle of Willis was detected. There was no gross evidence of tumour or mass lesion. Face and neck: Small superficial haemorrhage in the site of the abrasion on the nose with no fracture of the facial bones and no other soft tissue haemorrhages.

Figure 2: Base of the brain showing diffuse Subarachnoid Hemorrhage.

Figure 3: A- Surface of the brain after removal of blood clots showing circle of Willis (arrow) with ruptured aneurysm. B- Circle of Willis with ruptured berry aneurysm and Whitish Plaques (Atherosclerosis).
Chest: The heart weighed 640 gm. Grossly, asymmetric cardiac hypertrophy and atheromatous patches were noted (Figure 7). The interventricular septum and the left ventricular walls were hypertrophic. Transverse section of the left ventricle revealed concentric hypertrophy (Figure 9) also, the thickness of the left ventricular wall was 28 millimetres. The septal thickness was 30 millimetres. When dissecting the coronary arteries, we observed moderate to severe degree of atherosclerosis of the left coronary artery (main-stem) and its left anterior descending (L.A.D.) branch shows 60% occlusion, while left circumflex artery shows 25% occlusion and right coronary artery shows 10%occlusion (Figure 8a,b,c). Lung examination showed no abnormalities. Also, the autopsy of the abdomen and pelvis showed no fracture of bones and no soft tissue haemorrhages.
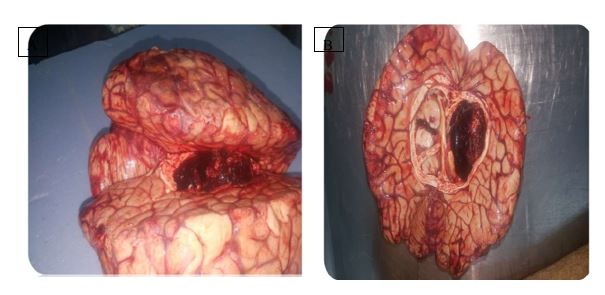
Figure 4: A-Brain showing intraventricular and intracerebral hemorrhage. B- A cross section of the brain showing abundant blood filling the entire ventricular system.
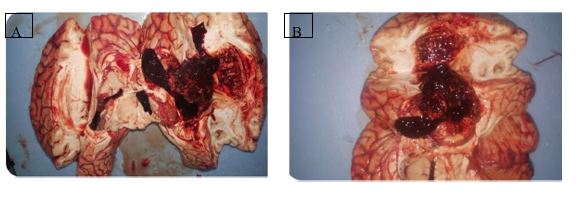
Figure 5: A&B- Cross sections of the brain showing intraventricular and intracerebral haemorrhage.
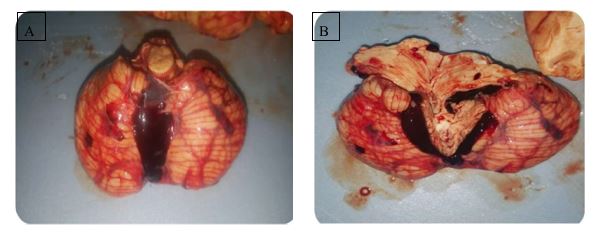
Figure 6: A- Brain stem and cerebellum & B- cross section: showing pontine and cerebellar haemorrhage.
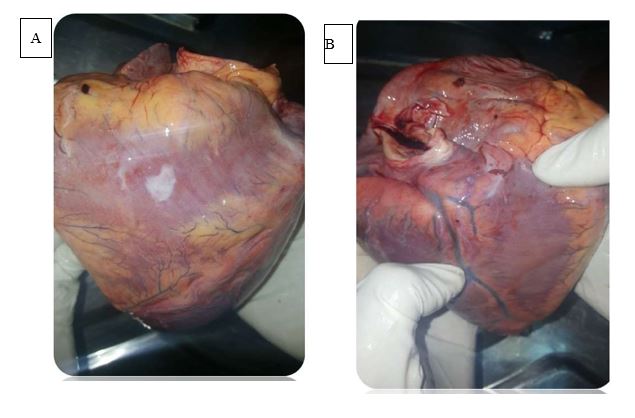
Figure 7: A&B- Heart weighed 640 gm showed asymmetric hypertrophy and atheromatous patches.
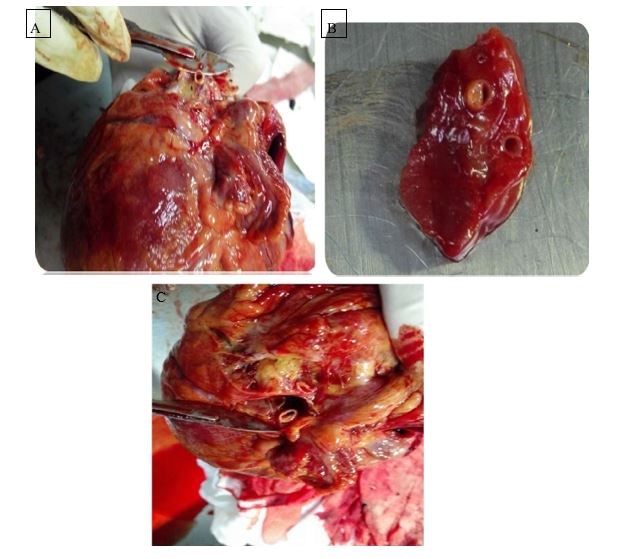
Figure 8: Figure 8: Dissecting the coronary arteries showing: A- Left circumflex artery with 25% occlusion B- left anterior descending (L.A.D.) branch with 60% occlusion. C-right coronary artery with 10% occlusion.
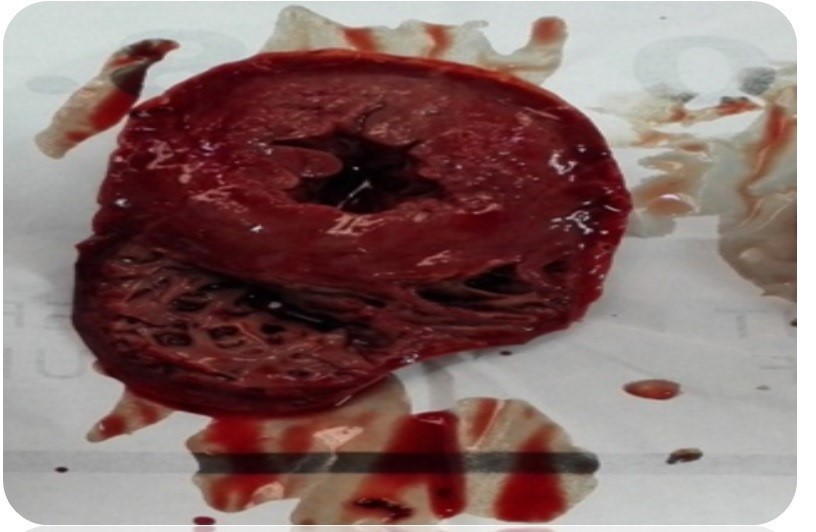
Figure 9: Transverse section of left ventricle showing concentric hypertrophy.
Forensic investigation
There were no other abnormal findings. X-ray was done for the whole body and didn’t reveal any fracture or foreign bodies. Laboratory investigations were done to show if there was any drug was taken to assist or cause death. A urine drug screen was done and revealed negative results for the drug of abuse (Figure 10).
Figure 10: Urine drug screen results showing negative results for the drug abused.
Forensic photography
The autopsy was performed with the direct permission of the prosecutors in the morgue of Forensic Medicine Authority and the major autopsy findings were documented properly through photography by using a digital camera.
Discussion
We have described a fatal case of intracranial haemorrhage caused by a ruptured aneurysm at the circle of Willis in association with undiagnosed hypertension. An aneurysm is defined as an abnormally dilated segment of a blood vessel. Berry aneurysm is by far the commonest of all cerebral aneurysm. About 25% of cerebrovascular deaths are due to its rupture [5]. Berry aneurysms, also known as saccular aneurysms, are sac-like out-pouching in the cerebral blood vessels, which appear berry-shape on external examination, therefore the name. Aneurysms usually reside in the Circle of Willis [6]. Berry aneurysm can rupture at any time, during exertion or at rest. Rupture of this aneurysm ends in haemorrhage in subarachnoid space and occasionally in brain parenchyma. The most common pattern noted is subarachnoid haemorrhage alone, but haemorrhages in other areas are fairly common [2-7]. The presented case reiterates the fact that the causes of non-traumatic intraparenchymal and subarachnoid haemorrhage are in 10% of cases consistent with a ruptured berry aneurysm [3]. The pathogenesis of berry aneurysm formation is multi-factorial. The risk factors for developing berry aneurysms include any condition that causes hypertension, including atherosclerosis [8]. All studies to date show peaks at various ages in the 40-70year range, which is consistent with our case where the age of the deceased is 40 yrs [7]. The pathological findings of the presented case including concentric left ventricle hypertrophy, moderate to severe atherosclerosis of coronary arteries which are consistent with hypertensive heart disease. The rupture of the aneurysm is thought to be a consequence of a rise in blood pressure that occurs in this situation. Moreover, hypertensive heart disease could explain the presence of different types of intracranial haemorrhage rather than only subarachnoid haemorrhage which is considered the usual presentation of a ruptured berry aneurysm.
When evaluating cases of apparent sudden death consideration must be given to whether pathology found has caused death or is incidental. A person may die with, but not from, disease [9]. Typically, a spontaneous subarachnoid haemorrhage is indicated by a sudden, severe headache, frequently accompanied by nausea, vomiting, and dizziness. Loss of consciousness occurs in about half the cases of spontaneous haemorrhage. Neurologic symptoms may include partial paralysis, loss of vision, speech difficulties, and seizures. Seizures result from the sudden rise in intracranial pressure or direct cortical irritation by blood [10]. These symptoms could explain the falling of the deceased on the bathroom and the presence of external injuries and the dark blue hypostasis founded on the external examination of our case.
Conclusion
Intracranial haemorrhage is an occasional finding at autopsy in cases of sudden, nontraumatic death. In some cases, the cause of such haemorrhage is grossly visible such as ruptured berry aneurysm. The cause of death was due to rupture of berry aneurysm at the circle of Willis which resulted in subarachnoid haemorrhage in addition to intraventricular and pontine haemorrhages with underlying hypertensive and atherosclerotic cardiovascular disease the manner of death was natural. However, the diagnosis of massive subarachnoid and cerebral haemorrhages is self-evident. But the large amounts of freshly formed blood clot make it is often difficult to locate the berry aneurysm. So, it is vital to examine the brain while it is still fresh. Moreover, the subarachnoid membrane should be removed with forceps and the surface of the brainwashed with isotonic saline before fixation with formalin.
Key points
1. A systematic autopsy is an important part of the diagnosis of a ruptured berry aneurysm. In cases, where the death of the individual is due to intracranial haemorrhage, the issue for the Forensic pathologist to rule out unnatural causes.
2. During an autopsy, the presence of intracranial haemorrhage accompanied by evidence of trauma like scalp contusion/fracture of skull bone excludes the natural causes.
3. The common cause of berry aneurysm is hypertension and atherosclerosis which make the vessel prone for rupture. In such circumstances, even the minor trauma to the head could cause bleeding leading to the death of the individual.
4. Ruptured aneurysms must be considered as a probable cause of death in bodies brought for autopsy where findings revealed subarachnoid and /or subdural haemorrhage with no external trauma. Dissection of the cerebral vessels is essential for diagnosis, particularly when deaths are unexpected in nature. This can be very important each for the family to know the cause for his or her loved one's death and conjointly for any legal or insurance reasons which will follow.
5. Sudden adult death scene investigation requires the interrogation of the witnesses and family members of the deceased. In addition, recent symptoms before death and past medical history must be looked for.
Compliance with ethical standards
Ethical approval: This article does not contain any studies involving human participants or animals performed by the authors. Informed consent: Informed consent was obtained from the decedent’s wife.
References
- De la Grandmaison GL. 2006. Is there progress in the autopsy diagnosis of sudden unexpected death in adults? Forensic Sci. Int. 27: 138-144.[Ref.]
- Black M, Graham DI. 2002. Sudden unexplained death in adults caused by intracranial pathology. Journal of clinical pathology. 55: 44-50.[Ref.]
- Tomcik MA, Gerig NR, Prahlow JA. 2011. Sudden death from ruptured intracranial vascular malformation. Forensic science, medicine, and pathology. 7: 185-91.[Ref.]
- Itabashi H H, Andrews J M, Tomiyasu U, et al. 2011. Forensic neuropathology: a practical review of the fundamentals.[Ref.]
- Perry A, Brat DJ. 2010. Practical Surgical Neuropathology- a diagnostic approach. Philadelphia, Churchill Livingstone. 539.[Ref.]
- Gasparotti R, Liserre R. 2005. Intracranial aneurysms. European radiology. 15: 441-447.[Ref.]
- Punitha R, Kumar MV, Rayamane AP, et al. 2014. Natural Intracranial Hemorrhage and Its Forensic Implications: A Case Review. Journal of Indian Academy of Forensic Medicine. 36: 215-217.[Ref.]
- Shkrum, MJ, Ramsay D A. 2007. Forensic pathology of trauma. Springer Science & Business Media. 607-622.[Ref.]
- Langlois N E. 2009. Sudden adult death. Forensic science, medicine, and pathology. 5: 210-232.[Ref.]
- Cvetkovi? D, Živkovi? V, Nikoli? S. 2016. Unusual appearance of facial petechiae and conjunctival hemorrhages: the trout phenomenon in a case of fatal subarachnoid hemorrhage due to ruptured berry aneurysm. Forensic science, medicine, and pathology. 12: 520-522.[Ref.]


















