
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Research ArticleDOI Number : 10.36811/ijfs.2019.110007Article Views : 16Article Downloads : 24
Sexual Assault Forensic Examination in adult and child cases: Is Colposcopy Really Necessary?
Eman Ahmed Alaa El-Din1*, Maha Hasanin Kamel2, Azaa sobhy1, Sahar Abd El Rasheed1 and Mohamed Salah Abdelkhalek2
1Department of Forensic Medicine & Clinical Toxicology, Faculty of Medicine, Zagazig University, Zagazig, Egypt
2Egyptian Forensic Medicine Authority, Cairo, Egypt
*Corresponding Author: Eman Ahmed Alaa El-Din, Associate Professor of Forensic Medicine and Toxicology, Departments of Forensic Medicine & Clinical Toxicology, Faculty of Medicine, Zagazig University, Egypt, Tel: +201226026944; Email: Eman_alaa77@yahoo.com
Article Information
Aritcle Type: Research Article
Citation: Eman Ahmed Alaa El-Din, Maha Hasanin Kamel, Azaa sobhy, et al. 2019. Sexual Assault Forensic Examination in adult and child cases: Is Colposcopy Really Necessary?. Int J Forensic Sci. 1: 45-58.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2019; Eman Ahmed Alaa El-Din
Publication history:
Received date: 09 October, 2019Accepted date: 15 October, 2019
Published date: 18 October, 2019
Abstract
Sexual assault is a complex situation with medical, psychological, and legal aspects. Victims should be examined by a specially trained medico-legal examiner to collect evidence and avoid multiple examinations. The use of colposcopy in child and adult sexual assault cases is becoming increasingly more widespread however; it is still not a routine aspect of all examinations in most countries. The present study aimed to evaluate the importance of using the colposcope in the examination of the sexual assault cases admitted to the violence against women and child clinic in the Forensic Medicine Authority in Egypt. The study included (150) cases, divided into two groups according to age: Group A (1 to 18 years) (124) male and female children and Group B (19-40 years) (26) females. -General, then local examination with the naked eye and colposcopy had been performed. Internal genitalia was examined by using disposable plastic Casco in adult non-virgin victims only. -Vaginal and anal swabs were collected for the detection of seminal stains. The results of the colposcopic examination revealed a significant difference in both negative and positive results when compared to the other methods of examination (naked eye, swabs, and clothes examination). Colposcopic magnification power with high resolution and illumination light permits to discover microtrauma which may not be discovered with a normal examination by naked eyes. Colposcope seems to be an important noninvasive tool for the examination of children and adults when sexual abuse is suspected. Its documentation could allow for supervision, teaching, and second opinions in an ethically difficult setting. The colposcopic examination should be introduced to all forensic departments in Egypt to be used as a routine aspect of all sexual assault examinations. Future studies are recommended to be conducted on a national scale.
Keywords: Sexual assault; Colposcope; Toluidine blue dye; Examination
Introduction
Sexual assault is usually under-reporting for several reasons; including the feeling of shame, disbelief, besides, the majority of cases have both violence and sexual abuse. The definition of the forms of violence differ broadly from one country to another, many countries have no good reporting system to determine the prevalence of different types of violence facing women and children. The failure to investigate and expose the true extent of violence allows governments, families, and communities to ignore their responsibilities [1]. Suitable attention and care are needed for the victims of sexual assault. A lot of changes faced the forensic examiners regarding the responsibility of dealing with victims and providing effective measures and preventive setting. The most stressful task is to prove the assault and to undertake correct documentation and collection of evidence [2,3]. A genital injury is a type of trauma that has happened as a result of physical contact. If any abnormality is seen on examination, the first forensic priority is to evaluate its nature to differentiate between true injury and other pathological causes like infection, inflammation, bleeding disorder, skin disease or cancer [4].
Using modern techniques like colposcope with its video recording facilities in the examination of genital injury and recording of physical signs utilizing high-quality photographs would improve practice sexual assault examination and give the perfect care to sexual abuse victims [5]. Therefore, it is considered a golden standard practice in the United Kingdom for the examination of both adults and children, whereas in Australia colposcopic examination is used only in the young [6]. The colposcopic examination is vital to be done when injuries are not seen by an unaided eye examination and when we need to save the photos as a piece of evidence to be used later for jurisdiction [7,8]. The main advantage of the colposcopic examination of sexual assault victims is the single examination in one set and to avoid the need for several examinations or the presence of multiple examiners. Currently, most sexual assault research projects need photographic documentation of all findings to confirm that inter-observer reliability is sustained and the decisions meet the accepted standards of diagnosis [9]. The present study was designed to evaluate the importance of using the colposcope in the examination of the sexual assault cases of females and children admitted to the violence against women and child clinic in the Forensic Medicine Authority in Egypt.
Subjects and Methods
A-Subjects:
The study was carried out on 150 forensic medico-legal sexual assault cases (124) child and (26) Adult female) which had been examined in the newly established unit of the violence against woman and child in the main building of the Forensic Medicine Authority in Cairo, Egypt from February 2017 to 2018. The study protocol was approved by the Institutional Review Board (IRB) of the Faculty of Medicine, Zagazig University. Ethical considerations and confidentiality were respected.
Grouping of the cases: Cases divided into two groups according to the age.
1-Group A: (1to 18 years) No (124); 2-Group B: (from 19 up to 40 years) No (26).
Inclusion criteria: females with a recent history of sexual assault and male child have a recent history of sodomy. Exclusion criteria: Cases during menstruation or with a history of sexual assault more than two weeks or pregnant cases due to sexual assault for more than two weeks or with recent delivery after pregnancy from sexual assault. Also, trauma-related severe illness attributed to violence related to sexual assault not examined and referred to the hospital.
B-Methods:
Identification of the victim was done by personal identification card in adults and by taking fingerprints of young victims. Consent was taken from the cases for (examination- photography- evidence collection), informed consent was obtained from adult victims and the relatives of the first or second degree in case of child victims while the examination was conducted with the direct permission of the prosecutors in cases of mental retardation and children without families.
According to WHO (2003) [10], the steps of examination were explained to the victims, Complete history taking which includes: name, age, occupation, residency, marital state, and previous diseases. History of assault: complete detailed history including time type of act, instruments used, site, number of injuries, and post-incident of the event. History of treatment and management: All papers and reports of treatment, management, and investigation were analyzed in comparison to the history of attack. The questioning is followed by a complete forensic medical examination. During the examination, the victim is undressed and stands on a white sheet.
- A General examination was performed for the detection of evidence of general violence. Examination of body hair by a disposable comb for any retained hair from the assailant. Examination of the whole body for trauma and clothes for biological fluids by using UV rays then the clothes referred to the lab for detection of biological fluid. While victims with washed clothes were excluded from clothes examination [11].
-Local examination:
1- Naked eye examination of the external genitalia, inner thighs, and anus and recording of all findings, positive or negative.
2- Colposcopy of the external genitalia using a KAPS video-colposcope a high-quality German manufactured microscope from Karl Kaps [12]. The colposcopic examination was performed with the victim in both the back position (supine position) and the knee-elbow position. Digital photography using the integrated camera of the colposcope [13].
3-Toluidine blue dye was applied to the external genitalia and removed with 1% acetic acid after drying.
-Internal genitalia examination: Perineum, hymen, vagina, and anus for any tear and bruises by using disposable plastic Casco in adult non-virgin victims only [14].
-Samples collection: Vaginal and anal swabs were taken on special trial swabs and dried at room temperature then sealed in special tubes with a complete chain of custody then referred to the forensic laboratory to be investigated for detection of seminal stains; it is time-dependent, within seven days from the assault. So, victims with a history of assault more than one week were excluded from swabs examination [15].
Statistical analysis
The results were recorded, tabulated and statistically analyzed by excel system and statistical package for social sciences version 17.0 (SPSS) to show the relationship between each variant and the other in cross tables. Student t-test and Chi-square were done to show the degree of significance of the results. Chi-Square (X2) test was used for comparison between groups, determine whether there is a significant difference between the expected frequencies and the observed frequencies in one or more categories. P-Value was considered to be statistically significant if ≤ 0.05 [16].
Results
The study enrolled 150 sexual assault cases. Group (A) (1-18 years) included 124 victims, constituted (82.7%), while there were 26 cases in the group (B) (19-40 years) representing (17.3%). Regarding sex of examined cases, females constituted (64%): Seventy female cases (73%) were in the group (A) and 26 cases (27%) were in the group (B), while males were only (36%). The incidence of reported cases increased among the young age, especially in female cases. Regarding the form of the sexual assault; in female victims, there were (47.9%) had penile-vaginal penetration, (26%) had penile-anal penetration, (14%) had digital vaginal penetration, (7.3%) had digital anal penetration and (43.8%) of all female cases had complete penetration associated with ejaculation from the assailant. while in male cases (58%) had penile-anal penetration and (10%) had digital anal penetration. (32%) were positive for assailants’ejaculation (Table 1).
|
Table 1: The different forms of sexual assault in relation to sex. |
||||||
|
Forms of sexual assault |
Sex |
χ2 |
P
|
|||
|
Male (n=54) |
Female (n=96) |
|||||
|
n |
% |
n |
% |
|||
|
Penile vaginal penetration (n=46) |
0 |
0.0 |
46 |
47.9 |
37.3 |
0.000* |
|
Penile anal penetration (n=64) |
39 |
72.2 |
25 |
26.0 |
30.1 |
0.000* |
|
Digital Vaginal penetration (n=14) |
0 |
0.0 |
14 |
14.6 |
8.69 |
0.003* |
|
Digital anal penetration (n= 14) |
7 |
12.9 |
7 |
7.3 |
1.31 |
0.252 |
|
Penetration with ejaculation (n= 64) |
22 |
40.7 |
42 |
43.8 |
0.128 |
0.721 |
|
P: significance (p <0.05 significant*) |
||||||
The most common form of sexual assault in age group (A) was penile-anal penetration (47.6%) cases, followed by penile-vaginal penetration (26.6%) while in the adult group (B) there was (50%) had penile-vaginal penetration followed by penile-anal penetration (19.2%). (41.1%) was positive for assailant ejaculation in the age group (A) while it was positive in (50%) of the group (B). Results showed a significant correlation between different forms of sexual assault and sex and age of the victims in this study (Table 2).
|
Table 2: The different forms of sexual assault in relation to age groups. |
||||||
|
Forms of sexual assault
|
Age |
χ2 |
P
|
|||
|
Group(A) 1-18y (n=124) |
Group (B) 19-40y (n=26) |
|||||
|
n |
% |
n |
% |
|||
|
Penile vaginal penetration (n=46) |
33 |
26.6 |
13 |
50.0 |
5.53 |
0.019* |
|
Penile anal penetration (n=64) |
59 |
47.6 |
5 |
19.2 |
7.06 |
0.008* |
|
Digital Vaginal penetration (n=14) |
12 |
9.7 |
2 |
7.7 |
0.100 |
0.752 |
|
Digital anal penetration (n= 14) |
14 |
11.3 |
0 |
0.0 |
3.24 |
0.072 |
|
Penetration with ejaculation (n= 64) |
51 |
41.1 |
13 |
50.0 |
0.691 |
0.406 |
|
P: significance (p <0.05 significant*) |
||||||
The results of the methods used for of examination showed that (14.7%) had positive findings for sexual assaults during the naked eye examination while in the colposcopic examination there were (68%). There was a significant increase in the rate of injury detection using a colposcopic examination. Also, in (53.3%) cases, injuries could not be detected by the naked eye while these faint injuries were detected by colposcopy after using high zoom and color filters (Figures 1-11).
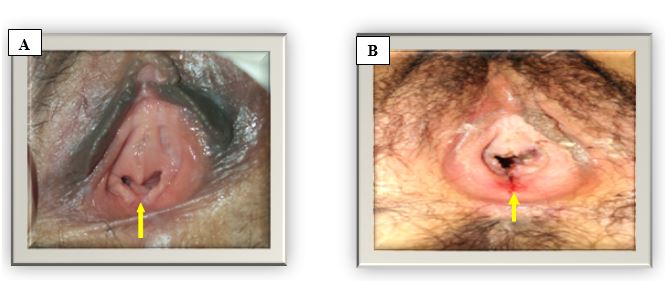
Figure 1: Colposcopic photographs showed: A- An old hymenal tear with healed edges at 6 o’clock, in an adult victim, the color change of the trauma and healing of the hymnal tear dating with the story of two weeks ago. B- Recent hymnal tears of adult case at 2 and 6 o’clock with red and edematous bloody edges.
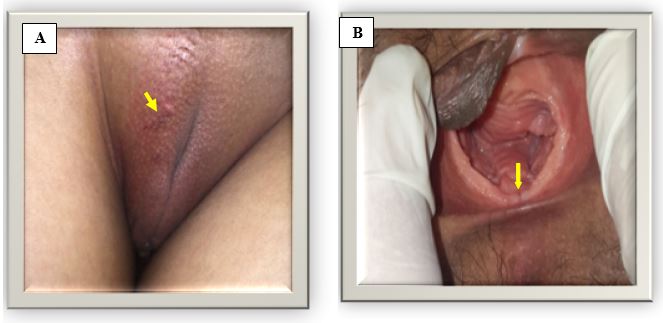
Figure 2: Colposcopic photographs of an adult victim of sexual assault showed: A-Recent scratch and redness on the labia majora. B- Dilatable and stretchable hymen a recent minute bruise at 6 o’clock without a tear of the same victim.
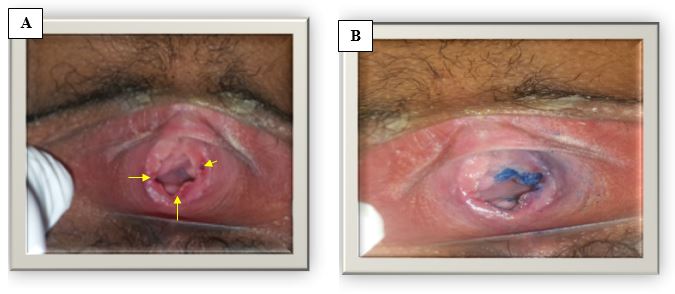
Figure 3: Colposcopic photographs of an adult victim of sexual assault Showed: A- Recent incomplete tears in the hymen at 2, 6 and 9 o’clock with edematous bruised edges. B- The same case after using toluidine blue dye in confirmation of the injury sites and it is absorbed in the mucous membrane of the vagina and hymenal tears.

Figure 4: Colposcopic photographs of an adult victim of sexual assault showed a recent superficial injury in the inner of the left labia majora caused by the nail of the assailant's finger.

Figure 5: Colposcopic photographs of an adult victim of sexual assault showed recent hymenal tears at 5 and 9 o’clock of the adult victim.
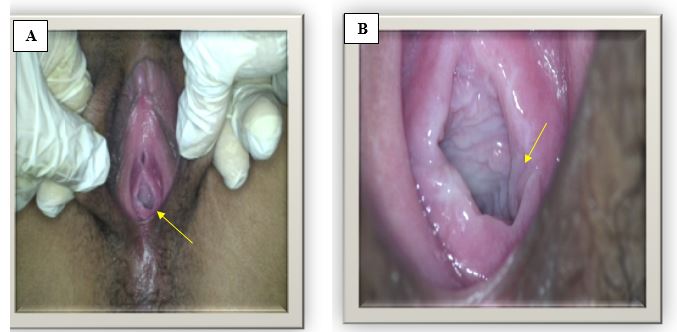
Figure 6: Colposcopic photographs of a suspected adult case of sexual assault showed: A- A suspected tear in the hymen at 5 o’clock at the examination. B- The high zooming power and focusing of the colposcope help in the detection of a hidden fold of the hymen which was suspected to be a tear at 5 o’clock of the same case.
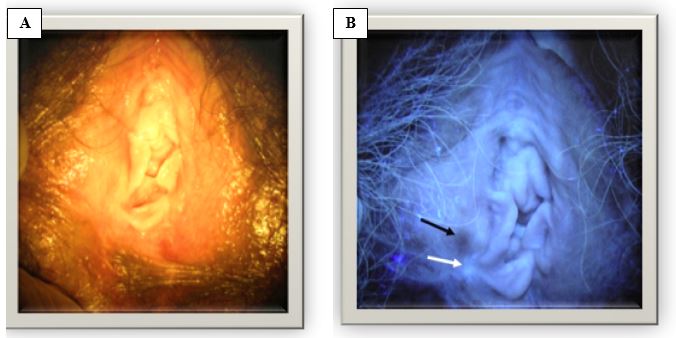
Figure 7: Colposcopic photographs of a non-virgin adult victim of alleged sexual assault A- No injuries or bruising could be detected by using ordinary light B- ultraviolet with specific wavelength beam light used for examination of the same case showed a hidden bruise.
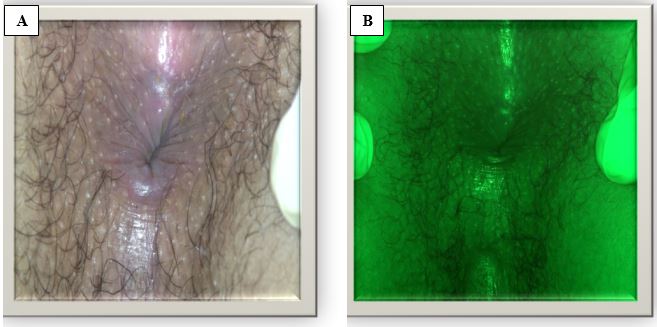
Figure 8: Colposcopic photographs of an adult victim of sexual assault showed: A- A free anal area before using the green color diaphragm tool. B- The same case by using the green color diaphragm to detect any hidden bruises.
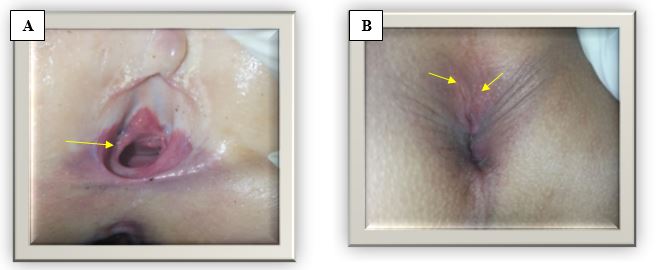
Figure 9: Colposcopic photographs of a 3 years female child victim of sexual assault showed: A- A trial to penetrate the hymen with bruises. B- The same case with two recent anal fissures at 12, 1 o’clock in the knee-chest position.
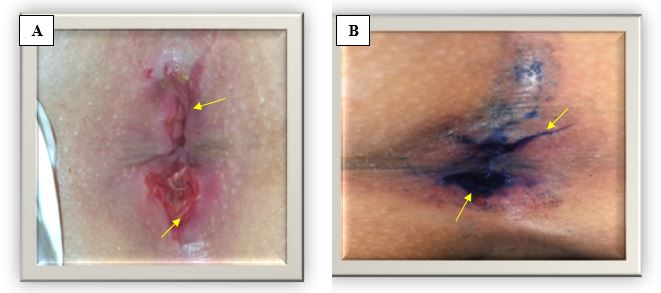
Figure 10: Colposcopic photographs of a male child victim of sexual assault showed: A- Severe deep anal fissures at 1 and 6 o’clock. B- The same case after using toluidine blue dye in confirmation of injuries sites showing the absorption of injured areas of the anal mucosa.
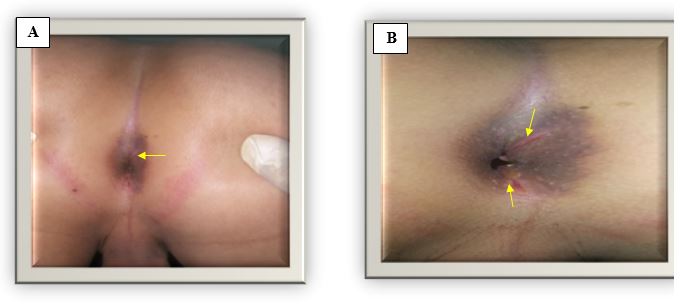
Figure 11: Colposcopic photographs of a 6 years old male victim sexual assault showed: A- A specific circular bruise around the anus. B- The same case with two anal fissures at 1 and 6 o’clock.
There was a statistically significant difference between the naked eye and colposcopic examination results at pvalue=0.000 (Figure 12). Vaginal and rectal swabs were taken from only forty-one cases who reported sexual assaults in the first week; (39%) was positive for seminal stain while (61%) was negative. Also, the clothes of sixty-three cases whose clothes had been kept without washing, the results of the examination showed that (50.8%) were positive for seminal stains while (49.2%) were negative. There was no significant difference between the results of swabs and cloth examination. There was significant importance for both positive and negative results of colposcopy examination in correlation to the results of swabs and clothes examination.
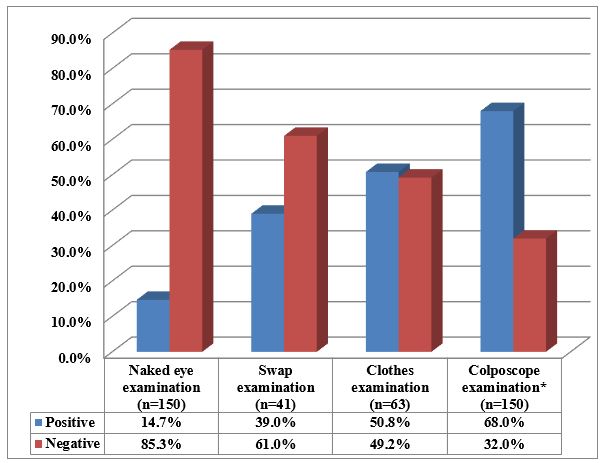
Figure 12: Graph showing comparison between the results of the colposcopy examination and the other methods of examination in sexual assault cases.
*chi-square = 89.4, p-value = 0.000
Discussion
The prevalence of sexual abuse among women and children, in general, has been fairly documented to some degree, but until recently this problem has received very little attention in developing countries [17]. The key official response to sexual violence has been centered on the creation of supportive evidence to be used in investigative and judicial proceedings. Which made a forensic medical examination vital for sexual assault cases [18]. Using direct visualization only for sexual assault examination does not prove an adequate approach to notice all injuries. Accordingly, introducing new techniques as the colposcopy examination could give accurate and satisfactory results. Therefore, the current study attempted to highlight the importance of colposcopic examination of sexual assault cases. The present study had documented a higher incidence of reported cases of sexual assault among group A (1 to 18 years). Also, a higher percentage of female cases, (73%) versus (27%) in the older age group (B) were recorded. Committee on Health Care for Underserved Women (2014) and Vrees (2017) [19,20] stated that adults' under-reporting of sexual assault may be due to the fear of shame, skepticism, community traditions and fear of divorce in married victims or loss of work in working one. Or maybe the adult victims had children and fear from sham for them too. Also, the under-reporting from male victims conceded with Ernst et al., (2000) [21] who reported that many of the male sexual assault victims did not seek care and fear from the stigma as homosexual or fear the embarrassment of examination in a hospital setting. The present study detected different types of sexual assault in the examined cases. The most common type of sexual assault in age group (A) was penile-anal penetration in (47.6%) followed by penile-vaginal penetration in (26.6%) while in the older age group (B); (50%) had penile-vaginal penetration followed by (19.2%) had penile-anal penetration. Forty-one percent of cases showed positive findings for assailant ejaculation in the group (A) while it was positive in (50%) in the group (B). These results were near to Riggs et al. (2000) [22] who mentioned that there were many types of genital injuries in victims of sexual assault, they reviewed files of 941 patients; 6% reported only finger-vaginal penetration. Localized injuries were discovered in 81% of the victims. There were about (3%) of the cases had digital anal penetration and about twenty percent of the victims were virgin and had a recent hymenal tear or no injuries at all in non-virgin adult victims (48%). Furthermore, Zilkens et al. (2017) [23] had studied the rate of genital and anal injury and assault characteristics in women alleging sexual assault in Western Australia. Whereas, a total of 1266 women were examined from Jan-2009 to Mar-2015. The genital injuries were found in 24.5% of all women who reported a completed vaginal penetration; in victims with no previous sexual intercourse, 52.1% had a genital injury, the anal injury was discovered in 27% of reported completed anal penetrations, in the cases with previous vaginal intercourse there were a big portion of the victims with no genital injuries during assault. Regarding, the role of colposcopy examination in the detection of sexual assault injury in the current study, there was a statistically significant increase in the positive result by using the colposcope versus the unaided eye examination. Whereas (14%) of cases had positive findings during naked eye examination while in the colposcopic examination (68%) showed positive findings. These results were in agreement with Yung, (2015) [24] who reported that colposcope improves detection of genital trauma in victims of sexual assault compared with gross visual examination alone. He conducted a prospective one month pilot study of seventeen female sexual assault victims. He observed that using the colposcope permit the documentation of sexual assault injuries in nine cases from seventeen one which considered as (53%), compared with only one case from the seventeen was proved to have genital injuries when examined with the naked eye and the colposcope improve the detection of the victim's injuries. The present study showed no significant differences between the results of genital swabs and the samples taken from the cloths of the victims. Swabs were taken from forty-one cases examination revealed that there were seventeen cases (41.5%) positive while twenty-four cases (58.5%) were negative for seminal stain. While the results of the clothes examination revealed that thirty-four cases (54%) were positive while twenty nine cases (46%) were negative for seminal stains detection of the assailant. Sena et al. (2015) and Thackeray et al. (2011) [25,26] discussed the importance of physical evidence to prove the act of sexual assault and confect the assailants in cases of sexual assaults. Semen, blood, vaginal secretions, saliva, vaginal epithelial cells, and other biological evidence may be identified and profiled by a forensic lab. Physical evidence must be collected as fast as possible with qualified personnel and preserved properly to give the chances for a successful criminal prosecution in the future.
The sexual assault can be proved by the investigation and can even determine if it happens or not, and the results of the analysis can be preserved for a long time for correlation with suspected assailants and make identification and comparison between assailants’ samples and evidence collected from the victims [27]. The results of the current study coincided with Ernst et al. (2010) [28] who stated that in victims of sexual assault, colposcopy was better for the detection of additional genital trauma than gross examination. Protocols involving conventional methods without colposcopy historically led to detect a genital finding in 10% to 30% of female sexual assault victims, while this percentage elevated to be ranged between 87% to 92% when colposcope was used. Templeton and Williams (2006) and Rogers and McBride (2014) [29,30] mentioned that colposcopy is a clinical procedure used to examine the epithelium of anogenital area with a magnifying instrument by which microtrauma and mucosal surface injuries such as scratches, lacerations, edema hymenal tears, and anal cracks could be detected easily after both consensual and non-consensual intercourse and sexual attack. Also, it has good light sources and zooming powers that permit a detailed and accurate examination and gives the chance for noninvasive photos that do not need a flash illumination Sommers et al. (2005) and (Kesic, 2005) [31,32] had discussed that the positive results of swaps and cloths examination in sexual assault victims, while there was negative finding with the colposcopic examination, could be attributed to the timing of examination by colposcopy and healing of microtrauma or friction mark and disappearance of the redness in genitalia during external friction without penetration. Anal penetration did not result in visible anal injury in the majority of cases, the external anal examination may be not enough to be seen anal injury and anoscope may be needed. Newton (2013) [33] recommended to follow up the guidelines of the American Academy of Pediatrics for collecting forensic evidence and advised to collect the evidence within three days after the assault of sexual abuse. He studied the medical records of 273 sexual assault victims who were examined in hospital emergency departments and had forensic examination and evidence in about twenty-five percent of the victims, the forensic evidence was collected and identified in all who examined within forty-four hours from the assault. More than ninety percent of cases with positive finding was within the first day of the assault. Sixty-five percent of the evidence finding was collected from the victim's clothes. Conclusions: The colposcope seems to be an acceptable noninvasive tool for the examination of children and adults when sexual abuse is suspected. Colposcope will not replace the meticulous, sensitive, well-trained professional examiners, but it can bring the best of documentation and accurate diagnosis to support victims and assailants’ history that improving the objectivity of forensic evidence collection. The results of the current study were based on data and evidence collected from the reported cases only, while the non-reported cases were not known and may be great enough to change this view. According to the current study, the colposcopic examination should be introduced to all forensic departments in Egypt to be used during sexual assault examination. Also, future studies are recommended to be conducted on a national scale to obtain a comprehensive picture of this important issue in the Egyptian community aiming at building a system that can appropriately respond to the challenges of sexually and physically abused victims. There is an actual need to increase public awareness to encourage victims to report the assault with no fear of stigma and teach the victims how to preserve evidence.
Acknowledgement
Sincere appreciation is expressed to all members in Forensic Medicine and Clinical Toxicology Department and the Egyptian Forensic Medicine Authority for their encouragement and support.
References
1. Cone D, Brice JH, Delridge, et al. 2014. Sexual assault.In: Emergency Medical Services: Clinical Practice and Systems Oversight, 2 Volume. 430. Ref.: https://bit.ly/33zgW5P
2. Moylan CA, Lindhorst T. (2015) Institutionalizing an ethic of coordinated care for rape victims: Exploring processes of legitimacy and decoupling in sexual assault response teams. Social Service Review. 89: 138-165. Ref.: https://bit.ly/2OMjetW
3. Bows H. 2018. Practitioner views on the impacts, challenges, and barriers in supporting older survivors of sexual violence. Violence against women. 24: 1070-1090. Ref.: https://bit.ly/35xkMOm
4. Gnann JW, Whitley RJ. 2016. Genital Herpes. New England Journal of Medicine, 375: 666–674. Ref.: https://bit.ly/2MdTCEU
5. Larkin HJ, Cosby CD, Kelly D, et al. 2012. A pilot study to test the differential validity of a genital injury severity scale, in development for use in forensic sexual assault examinations. Journal of forensic nursing. 1: 30-38. Ref.: https://bit.ly/35xbiD2
6. Leeson SC, Alibegashvili T, Arbyn M, et al. 2014.The future role for colposcopy in Europe. Journal of Lower Genital Tract Disease, 18: 70-78. Ref.: https://bit.ly/35xbiD2
7. White D, Du Mont J. 2009. Visualizing sexual assault: An exploration of the use of optical technologies in the medico-legal context. Social Science & Medicine. 68: 1-8. Ref.: https://bit.ly/35xbRg8
8. Ernst EJ, Speck PM, Fitzpatrick JJ. 2012. The element of naturalness when evaluating image quality of digital photo documentation after sexual assault. Advanced emergency nursing journal. 34: 250-258. Ref.: https://bit.ly/2INZZfH
9. Ernst EJ, Speck PM, Fitzpatrick JJ. 2011. Usefulness: forensic photo documentation after sexual assault. Advanced emergency nursing journal. 33: 29-38. Ref.: https://bit.ly/32dJqll
10. World Health Organization. 2003. Guidelines for medico-legal care of victims of sexual violence. Ref.: https://bit.ly/2OLcsVf
11. Lincoln CA. 2018. Sexual assault: forensic examination in the living and deceased. Academic forensic pathology, 8: 912-923. Ref.: https://bit.ly/32oePSd
12. KAPS VICO Video Colposcope. DP MedicalSection, 2019, Available.at: colposcope [Accessed 16 Feb. 2019]. Ref.: https://bit.ly/2Mcb38u
13. Ludes B, Geraut A, Väli M, et al. 2018. Guidelines examination of victims of sexual assault harmonization of forensic and medico-legal examination of persons. International journal of legal medicine. 132: 1671-1674. Ref.: https://bit.ly/2OV98r1
14. Astrup BS, Ravn P, Lauritsen J, Thomsen JL (2012) Nature, frequency and duration of genital lesions after consensual sexual intercourse—Implications for legal proceedings. Forensic science international. 219: 50-56. Ref.: https://bit.ly/2qdTqNn
15. Alderden M, Cross TP, Vlajnic M, Et al. 2018. Prosecutors’ Perspectives on Biological Evidence and Injury Evidence in Sexual Assault Cases. Journal of interpersonal violence. Ref.: https://bit.ly/2ovjlzD
16. Norusis MJ. 2011. IBM SPSS Statistics 19 Advanced Statistical Procedures Companion. Manual Spss.444.
17. Pritchard J. 2013. Good practice in promoting recovery and healing for abused adults. Jessica Kingsley Publishers.28. Ref.: https://bit.ly/33xYEBB
18. Rosenstein JE, Carroll MH. 2015. Male rape myths, female rape myths, and intent to intervene as a bystander. Violence and gender. 2: 204-208. Ref.: https://bit.ly/2oH5yWt
19. Committee on Health Care for Underserved Women. 2014. ACOG Committee Opinion no. 592: Sexual assault. Obstetrics and gynecology. 123: 905. Ref.: https://bit.ly/2ovqsYP
20. Vrees RA. 2017. Evaluation and management of female victims of sexual assault. Obstetrical & gynecological survey. 72: 39-53. Ref.: https://bit.ly/33qwfO3
21. Ernst AA, Green E, Ferguson MT. 2000. The utility of anoscopy and colposcopy in the evaluation of male sexual assault victims. Annals of emergency medicine.36: 432-437. Ref.: https://bit.ly/32hbRi0
22. Riggs N, Houry D, Long G, et al. 2000 Analysis of 1,076 cases of sexual assault. Annals of emergency medicine. 35: 358-362. Ref.: https://bit.ly/33sVyPu
23. Zilkens RR, Smith DA, Phillips MA. Et al. 2017. Genital and anal injuries: A cross-sectional Australian study of 1266 women alleging recent sexual assault. Forensic science international. 275:195-202. Ref.: https://bit.ly/32fLau6
24. Yung CR. 2015. Concealing campus sexual assault: An empirical examination. Psychology, public policy, and law. 21: 1. Ref.: https://bit.ly/2nNoF0M
25. Seña AC, Hsu KK, Kellogg N, Girardet R, Christian CW, Linden J, Griffith W, Marchant A, Jenny C, Hammerschlag MR. 2015. Sexual assault and sexually transmitted infections in adults, adolescents, and children. Clinical infectious diseases. 61: S856-S864. Ref.: https://bit.ly/2pm4KXi
26. Thackeray JD, Hornor G, Benzinger EA, et al. 2011. Forensic evidence collection and DNA identification in acute child sexual assault. Pediatrics. 128: 227-32. Ref.: https://bit.ly/31hf7IR
27. Badour CL, Feldner MT, Blumenthal H. et al. 2013. Examination of increased mental contamination as a potential mechanism in the association between disgust sensitivity and sexual assault-related posttraumatic stress. Cognitive therapy and research. 37: 697-703. Ref.: https://bit.ly/2BchAdk
28. Ernst EJ, Speck PM, Fitzpatrick JJ. 2010. Photo documentation image quality scoring system in the evaluation of female genital injuries following sexual assault. Advanced Emergency Nursing Journal. 32: 272-281. Ref.: https://bit.ly/2VEQXH5
29. Templeton DJ, Williams A. 2006. Current issues in the use of colposcopy for examination of sexual assault victims. Sexual Health. 3: 5-10. Ref.: https://bit.ly/2MgIRlf
30. Rogers D, McBride BM. 2011. Sexual assault examination. In:Clinical Forensic Medicine, Humana Press. 71-131. Ref.: https://bit.ly/2MgIXJD
31. Sommers MS, Fisher BS, Karjane HM. 2005. Using colposcopy in the rape exam: Health care, forensic, and criminal justice issues. Journal of Forensic Nursing. 1: 28-35. Ref.: https://bit.ly/2MKDPfQ
32. Kesic VE. 2005. Colposcopy of the vulva, perineum and anal canal. CME Journal of Gynecologic Oncology.10: 85. Ref.: https://bit.ly/2B6plRQ
33. Newton M. 2013. The forensic aspects of sexual violence. Best practice & research Clinical obstetrics & gynaecology. 27: 77-90. Ref.: https://bit.ly/2VEPL6J


















