
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Case ReportDOI Number : 10.36811/jcri.2019.110004Article Views : 2467Article Downloads : 37
A bull gore injury: a rare case report and review of the literature
Alegbeleye Bamidele Johnson
Department of Surgery, St Elizabeth Catholic General Hospital, Cameroon
*Corresponding author: Dr. Alegbeleye BJ, B.Sc (Hon.), M.B; B.S(Ib), MMCS, PHD, Department of Surgery, St Elizabeth Catholic General Hospital, Shisong, P.O Box 8, Kumbo- Nso Bui Division, Northwestern Region, Cameroon, Tel: +237-670628857; Email: drbalegbeleye@gmail.com
Article Information
Aritcle Type: Case Report
Citation: Alegbeleye BJ. 2019. A bull gore injury: a rare case report and review of the literature. J Case Rept Img. 1: 27-36.
Copyright:This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2019; Alegbeleye BJ
Publication history:
Received date: 10 February, 2019Accepted date: 15 February, 2019
Published date: 18 February, 2019
Abstract:
Background: Bull gore injuries are not common in a city set up but are common in the rural areas. The range of injuries varies from abdominal, chest, scrotal injuries which are quite different from the usual injuries seen in the emergency and casualty like road traffic injuries and stab injuries. We report a rare case of bull gore injury seen in a 38-year-old farmer, managed in this peripheral mission hospital one involving a stray domestic bull, its management as well as review of the literature. It is aimed that the knowledge gained from analyses of these injuries may be beneficial to other clinicians in general and also applicable to the management of similar injuries sustained in rodeo or agricultural settings.
Case Presentation: A 38-year-old male farmer of Kumbo origin, Northwestern Cameroon was seen at the emergency department after being hit by a stray domestic bull in his farm. He presented with a complaint of pain in the left iliac fossa, actively bleeding deep laceration in the left inguinal region and a left scrotal swelling. On presentation, his vital parameters (blood pressure: 120/80 mmHg, pulse rate: 82/minute, respiratory rate: 18/minute, temperature: 37.10 Celcius) were stable. On physical examination, the eviscerated left testes and cord was visible at the edge of a deep laceration in the left inguinal region and there was moderate swelling in the left iliac fossa. Rectal examination did not reveal additional finding. The bowel sounds were normal. We made a clinical diagnosis of penetrating abdominal injury with evisceration of left testes. The findings from the initial laboratory studies; Chest and plain abdomen radiographs were essentially normal. Focused abdominal sonography for trauma showed minimal free fluid in the left paracolic gutter and pelvis as well as diffuse hypoechoic mass (hematoma) of anterior abdominal wall essentially in the left iliac fossa. He was resuscitated on intravenous fluids, IV Ceftriaxone 1gm 12hourly, IV Metronidazole 500mg 8hourly, IV Paracetamol 1gm 8hourly. He also had anti-tetanus prophylaxis and was thereafter transferred to the OR. He had exploratory laparotomy, and left groin exploration; extensive left groin wound debridement with evacuation of hemoperitoneum, orchidopexy and wound closure over left pelvic as well as scrotal drains. The post-operative period was uneventful with optimal recovery. The patient was subsequently discharged on the seventh post-operative day and had since been seen in the surgical outpatient clinic at three weekly intervals for six months with satisfactory outcome.
Conclusion: Trauma due to animals especially those caused by bull horn could be life threatening as well as leave disability due to the site involvement. Early intervention and trauma surgery can be both lifesaving and could also prevent disability at a later stage. Management of bull gore injury can be challenging to the surgeon who needs have high index of suspicion for the diagnosis of this condition and take a call on type of management. Also, surgical repair of the injury is also difficult because of the complex anatomy and the less accessibility. There is an increasing priority for preventive measures to curtail such mishaps.
Keywords: Bull horn Injury; Abdominal Trauma; Bull-Fight; Goring; Evisceration
Introduction
Bull gore injuries are commonly seen in rural areas where people make their living rearing the livestock for domestic and farming purposes but are less commonly seen in an urban setting [1,2]. A bull is an uncastrated adult male of the species Bos taurus (cattle) which appears relatively more muscular and aggressive than the female of the species otherwise referred to as the cow [3]. The bull has long been an important symbol in many cultures, and plays a significant role in both beef ranching and dairy farming as well as in a variety of other cultural activities [4]. The bull is normally a docile and easily domesticated animal which may sometimes become angry for no obvious reason [2,5]. These animals therefore can cause serious injuries by their various appendages, especially horns. The commonest site of injury in bullhorn cases is the abdomen and perineal region; also the injuries predominantly occur on right side of abdomen [1,5]. The reason for perineal involvement is its anatomical configuration leading horn hook to engage and penetrate [6]. The injuries caused by horns of bulls, cows or buffaloes are of various shapes, sizes and directions and are goring in nature and violent [7]. Goring is taken when the bull horn penetrates deeply in the muscles as well as body cavities4. Goring is also described as a single injury which includes a mix of lacerated wound, contusion and infection by many researchers [6,7]. The wounds produced are contusions, lacerations, penetration of body cavities and rarely fractures. Mostly subcutaneous tissues and muscles are affected but visceral injuries are also quite frequent. The maximum numbers of injuries are sustained in villagers while rearing the cows and bulls, during feeding, while tying them or milking the cows or buffaloes [7]. Fatalities resulting from injuries sustained due to bull goring are quite rampant owing to the lack of any specific guidelines for the same by the Corporation authorities. Bullfighting [1] is a very popular sport throughout Spain and in some parts of Latin America. It is also common in Southern India and till date remains a major source of injuries sustained from bull goring. There are only few reports of bull gore injuries in literature. Unfortunately, these injuries are infrequently reported. We report a rare case of bull gore injury seen in a 38-year-old farmer, managed in this peripheral mission hospital one involving a stray domestic bull, its management as well as review of the literature. It is aimed that the knowledge gained from analyses of these injuries may be beneficial to other clinicians in general and also applicable to the management of similar injuries sustained in rodeo or agricultural settings.
Case Presentation
A 38-year-old male farmer of Kumbo origin, Northwestern Cameroon was seen at the emergency department after being hit by a stray domestic bull in his farm. He presented with a complaint of pain in the left iliac fossa, actively bleeding deep laceration in the left inguinal region and a left scrotal swelling [Figure 1]. On presentation, his vital parameters (blood pressure: 120/80 mmHg, pulse rate: 82/minute, respiratory rate: 18/minute, temperature: 37.10 Celcius) were stable. On physical examination, the eviscerated left testes and cord was visible at the edge of a deep laceration in the left inguinal region. There was moderate swelling in left iliac fossa, with definite ecchymosis and mild tenderness but no rebound tenderness. There was no muscle guarding, no generalized tenderness or rebound tenderness over the whole abdomen. He also had moderate scrotal swelling and tenderness. Rectal examination did not reveal additional finding. The bowel sounds were normal. We made a clinical diagnosis of penetrating abdominal injury with evisceration of left testes. The findings from the initial laboratory studies including full blood count, urinalysis and electrolytes were essentially normal. Chest and plain abdomen radiographs were normal. Focused abdominal sonography for trauma (FAST) showed minimal free fluid in the left paracolic gutter and pelvis as well as diffuse hypoechoic mass (hematoma) of anterior abdominal wall essentially in the left iliac fossa. He was resuscitated on intravenous fluids, IV Ceftriaxone 1gm 12hourly, IV Metronidazole 500mg 8hourly, IV Paracetamol 1gm 8hourly. He also had anti-tetanus prophylaxis and was thereafter transferred to the OR. He had exploratory laparotomy, and left groin exploration. Operative findings were 500ml of hemoperitoneum, spleen, liver, small and large bowel were essentially normal, a viable left testes and cord structure, left abdominal wall hematoma with no traumatic hernia. He subsequently had evacuation of hemoperitoneum, extensive left groin wound debridement, orchidopexy and wound closure over a left pelvic drain and a scrotal drain. The intra-operative photogragh of hemaperitoneum is labelled as figure 2 while the immediate post-operative photogragh is labelled figure 3. The post-operative period was uneventful with optimal recovery. The patient was subsequently discharged on the seventh post-operative day and had since been seen in the surgical outpatient clinic at three weekly intervals for six months with satisfactory outcome.
Discussion
Bull gore injuries according are more commonly seen in rural areas of India and other developing countries [8-11]. Dogan et al in a study of injuries in animal husbandry concluded that bull gore injuries are the most common ones [9]. Bull horn impact injury can vary from contusions, lacerations and penetrating wounds involving internal organs. The injuries occur more commonly on the abdomen and perineum [9-11]. Murali et al in their case report of 2015 submitted that stray cattle and bull are quite rampant in India and Africa [12]. There have been injuries reported from these stray cattle also from other literature [1,2,12]. They wander in the city, block traffic and defecate on roads and most importantly attack people and at times gore people to death [1,2,12]. In a related development, bull horn injuries are very frequent, especially in areas with a strong bullfighting tradition - professional or amateur all over the world [13]. Wounds caused by bull horns present their own peculiarities that make them different from any other type of injuries as stated below [13].
Peculiarities of Bull Horn Injuries [13]
i. Presence of large tissue damage
ii. Different paths of injuries-cavities, twists and turns
iii. Cul-de-sac-also means a dead-end body tunnel
iv. Massive inoculation of aerobic and anaerobic germs as well as
v. The possibility of transmitting tetanus
Classifications of Bull Horn Wounds [13]
Bull horn wounds are classified into four different types:
1. Sideways thrust - where the horn thrusts the body tangentially causing only contusions
2. Jab - where the injury is caused by the tip of the horn
3. Misleading wound -where there is an orifice of entrance that is far from the core injury and where associated lesions can coexist
4. Goring - which is a deep wound that affects fascia and muscle
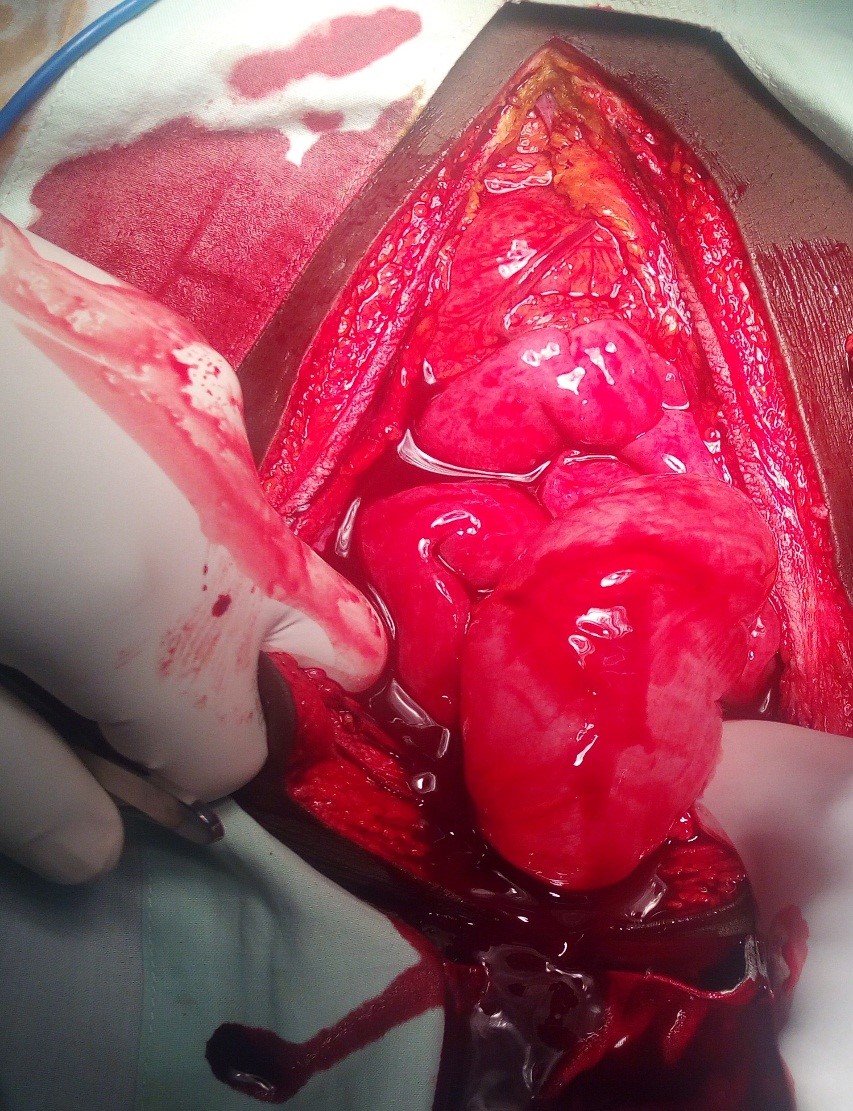
Figure 1: Eviscerated left testes and inguinal gore wound.

Figure 2: Intra-operative photogragh showing hemoperitoneum.
Sheathed goring’s is also known as “goring on healthy” and it occurs when the bull horn penetrates the body but, due to the elastic capacity of the skin, there is resolution of continuity and the skin returns to its previous appearance or shows mild alteration (ecchymosis, hematoma). The importance of this type of goring lies in the fact that during inspection and even during palpation, the presenting wound can be mistaken for a simple contusion [13-15]. Similarly, in our case, it was initially mistaken as a contusion over anterior abdominal wall, especially in the left iliac fossa. However, under a false appearance of mildness, injuries were extremely severe causing hemoperitoneum and required emergency surgery. In other related studies, the injuries are more commonly seen involving the abdomen and the perineum [1,2,9,13,16-19]. In the abdomen, the horn first tears the subcutaneous tissues and later muscles and further if the violence is more, the peritoneum is punctured [2,7,13]. Since the head of bull is at the same level as victim’s abdomen, this part of body is most exposed to the attack [2,11, 13]. The reason appears to be lack of bony shield over the abdomen permitting the horn hook to engage and penetrate [10]. In the bullring, the bullfighters most commonly sustain injuries on the abdomen for the same reason [13, 20]. These injuries can be in the form of perforations of abdominal wall, and internally hemorrhages and perforations involving mesentery and bowels [1,9,13].
Visceral injuries involving spleen and more frequently liver being situated on right region of the body are commonly encountered. Among the perineal injuries anovaginal fistula [9] urethrorectal fistula [6] injuries to anal canal and posterior vaginal wall have been caused by bullhorn. In our case the injury was on the abdominal wall and perineum, which is in concordance with other reports that the commonly injured region of the body being the abdomen. The obvious explanation is that the patient is an adult so the abdominal wall and perineum is at the level of the head of the cattle. The side involved was left side in contrast to commonly involved right side [16]. In all the above-mentioned studies, the larger frequency of injuries is located on right side [2]. The obvious explanation could be that the victim sustained injuries while rearing the animal, during feeding, tying to the poles, putting ropes round the neck and tying to the bullock-cart. During these maneuvers, the right side of body is exposed to the tip of the horn when the animal suddenly moves its head. Moreover, most of the people are right handed and the animal stands on the right side and hence the tip or body of the horn is in close association with the right side of the body. Other possible explanation could be that the victim may turn the right side of the body towards the animal protecting himself by using right arm in self-defense [10,11].
Injuries caused by bulls are dependent on socio-cultural characteristics of the society besides the ecology of the environment. In this sense, in Spain throughout the year particularly in the summer months the bulls’ participation is central to local festivities. In addition to bullfights in bullrings injured tend to be professional bullfighters. However, if bulls tend to run through the streets entertaining the inhabitants but killing many people including children that come in their way [20]. Indian continent is not at all immune to such celebrations. Singh et al [18] reported an unusual case of bull gore injury sustained during harvest festival celebrations in which the patient presented with blowout fracture of the orbital floor with metal horn cover and decorated ribbons impacted in the orbit.
Being gored by a bull in the abdomen is a most likely devastating and possibly fatal injury. These are the ultimate “snag” injuries that usually result in the runner being impaled with the weight of the body causing the horn to penetrate deeper into the tissues. The real danger comes if the horn penetrates through the abdominal wall and goes into the peritoneal or retroperitoneal cavities [21-22]. The most devastating area of injury would be to the retroperitoneal structures - duodenum, kidneys, aorta, vena cava, and pancreas. An injury to the aorta or vena cava would be immediately life-threatening in the fields after all [21-23].
Characteristics of Bull-Horn Wounds [13].
Bull-horn wounds are incisive and contusive, and they have special characteristics as below:
1. The entry opening is usually small and surrounded by an erosion zone
2. One or more in depth tracts may be present, usually with important muscular destruction
3. These wounds are contaminated, and multiple foreign bodies may be found at the bottom of the wound tract, including cloth fragments, dirt, and horn chips
The depth is dependent on the force of penetration of the bull’s horn into the body (which is the result of the animal’s weight and speed). There is an additional force because of the effect of the bull’s strong neck muscles when it raises its horns. This force causes upward tears at right angles to the ground. If the injured person is lifted, his body weight exerts an opposite force [22-24]. Finally, when the patient’s body is lifted and suspended by the bull’s horns, it is in an unstable balance which, depending on the location of the center of gravity relating to the horn, causes a rotational movement (with ensuing tears of arteries, veins, and nerves), combined with the animals efforts to disengage the person’s body [22-24]. In our case the direction of bull horn injury over anterior abdominal wall was upwards and laterally. Now the interesting fact in our case is that there was evisceration of the left hemiscrotum and cord structure which were viable enough to be returned by orchidopexy as well as the hemoperitoneum without accompanying bowel damage. Also, the gored left inguinal wound fortunately sparing the medial to left common iliac vessels [22-24]. Figure 3,4 are post -operative photographs of the index patient.
Figure 3: Immediate post- op photogragh.

Figure 4: Healing wounds in the index patient.

The problem of stray cattle and commonly the bull is a major health concerns in several undeveloped countries. They wander in some city, block traffic and defecate on roads and most importantly attack people and at times gore people to death. There is an urgent need for stringent guidelines should be formulated to preventing such mishaps in future. A number of researchers advocate wearing helmets and steel-toed boots as a simple and important safety strategy to prevent bull gore injuries [2,9,24]. Traffic police should take up this as civil responsibility to redirect and keep stray cattle away from road dividers and busy sections of the roads thus minimizing attacks. In addition, to prevent the animal from causing serious injury to humans, there is need for popularization of dehorning of domestic and stray cattle [2,23]. A more effective and prevalent method is local application of caustic potash when the calf is two months to two years old which eventually promotes dehorning [2,18]. Some literature has proposed other workers catching the stray cattle, restraining, or confining them in specially designated facilities to avoid human contact is an important step [2,9,23]. In one of such an effort to end stray cattle menace, the Governments of Delhi, Punjab and Gujarat have come up with various directives to be followed in this regard. Municipal Corporation of Delhi (MCD) is implanting microchip in the rumen of the animal that bears a unique Cattle identification number to help ascertain the cattle’s ownership and track their movement [2,25]. This would keep a check on illegal dairies and prevent smuggling of animal. In addition, MCD plans to impose a fine of Rs 5000 on the original buyer if an auctioned animal is rounded up. Moreover, it is expected of all and sundry to join hands to fight the menace of stray cattle on a common platform [2,25].
In a related development, Delhi High Court has ordered the Delhi government to cancel the license of any dairy or cattle shed if the cattle stray out of owner’s dairy or cattle shed. Under section 289 of the Indian Penal Code there is provision for prosecution of cattle owners whose cattle stray and roam about freely. Delhi High Court is following other stringent measures like disconnection of water and power supply to all illegal dairies and cattle sheds that are flourishing in the city [2,26]. Section 289 of the Indian Penal Code also guarantees an imprisonment for a period of six months to one year if the owner fails to prevent its cattle from causing any probable danger to human life or grievous hurt. In addition, Delhi High Court in July-August, 2005 directed the Delhi Police to make use of section 133 Criminal Procedure Court for removal of illegal dairies or cattle sheds [2,26]. This stringent legislation will in no little way reduce the menace of stray cattle in the long run both in India and other countries when fully implemented.
At this juncture, the lessons learnt from this case study could be summarized as follows. First, there is a very strong and urgent need for all cases of injuries from bull attacks in Kumbo-Northwestern Cameroon over the last 15 years be documented. In order to have an overview of the incidence, detail mechanism of injuries and management that could serve a prototype for policy makers as well as government actions. In many cases of bull attacks victims did not formally report their injury or did not even seek medical care within the neighboring farmers or packs; such persons need to be identified in the listings of incident reports. For every case collected as much data as possible: the victim's age and sex; date and circumstances of the attack; mechanism of injury and injuries sustained; location of medical care; treatment including any surgical intervention; antibiotic therapy and culture results; complications; and outcome.
This case report documents a direct person-to-bull contact. Many reports of automobile accidents caused by collision with or avoidance of a bull were found in the hospital case incident logs, but injuries to the vehicle occupants from such accidents were rarely noted. These details are not included in this study data. Also excluded were injuries sustained by individuals running or moving away from a bull without direct contact with the animal. The important lesson to the clinicians especially those involved in the care of such patients is to have high index of suspicion. Many bull gore injuries may not present as obvious injuries. The patient could have sustained major internal injuries like the index patient with hemoperitoeum etc. but still appears with normal clinical findings. In some documented reports present later with incisional hernias, anal fistula, and perineal abscess etc. The reason being that the skin is elastic and receive less impact than the deep internal organs during bull goring [2,10,18-20]. Therefore, there is a need for a high index of suspicion; followed by a detailed and thorough clinical physical examination, coupled with relevant radiological assessments by the attending clinician. Even in some instances, patient should be kept on admission and observation for a few days. In such cases, a patient with hemodynamic instability, fluctuating vital signs vis-a-vis tachypnea, tachycardia, hypotension will require close monitoring, further frequent reviews, early and prompt surgical intervention. In so doing preventing medical catastrophes for victims of bull gore injuries.
Conclusion
In rural Cameroon, bull remains a very useful animal for domestic and farming purpose. This domesticated animal surprisingly has caused life threatening injuries by accidental bull horn injury. The new knowledge gained from this case report and review of the literature is that one must look for and aggressively manage any such injuries after any encounter with bulls, and especially in the geriatric and younger population. Bull gore injury presents as a variety of bizarre and complex wounds. Familiarity with these lesions is important in areas where cattle are reared or where bullfighting is practiced. This is critical because of the unique characteristics they present in cases of trauma and wound management. Although bull horn wounds are severe, their prognosis is good, with few complications and a mortality rate of less than 1%. Following the basic ATLS principles can improve overall patient outcome.
Limitations of The Study
Lack of data-base on domestic animal injuries, inadequate reporting of such injuries, poverty, ignorance, and insufficient health infrastructure as well as level of skills of Clinicians in the sub-region of Cameroon are amongst the lists of possible limitations of this study.
Recommendations
1. There is a need for a data base of bull or domestic animal injuries in the region to contain the incidence, detail mechanism of injuries and management that could otherwise serve as prototype for policy makers as well as government actions.
2. Clinicians involved in the care of victims of domestic animal injuries require a high index of suspicion to preventing missed injuries and well trained on the basic ATLS principles so as to improve overall patient outcome.
3. A good understanding of the mechanism of injury and pathophysiology of bull gore injury is mandatory for all physicians.
4. Early intervention and surgical treatment is required to prevent further morbidity and mortality.
5. Effective government legislation on prevention of straying of cattle or other domesticated animal.
6. Finally, in resource constrained setting as ours, it is critical to raise awareness through public health campaign on prevention of this type of injury and improvement of existing health infrastructure.
Declarations
Availability of Data and Materials: Availability of data and materials confirmed by the Author.
Authors’ Contributions: BJA conceived of the study and participated in its design and coordination as well as helped to draft the manuscript; the author also read and approved the final manuscript.
Ethics Approval and Consent to Participate: Ethical approval not required for case reports at my institution.
Consent for Publication: Written informed consent was obtained from the patients for publication of this case report and any accompanying images. A copy of the written consents is available for review by the Editor-in-Chief of this journal.
References
- Wasadikar PP, Paunikar RG, Desmukh SB. 1997. Bull horn injuries in rural India. J Indian Med Assoc. 95: 3-4, 16. [Ref.]
- Rani M, Rohit, Sharma A, Dikshit PC. 2010. Injuries by bull horns: Patterns and prevention protocols. J Forens Med &Toxicology. 11: 1-26. [Ref.]
- Delbridge A. 1991. Macquarie Dictionary, The Book Printer, Australia. [Ref.]
- Sheena Coupe (ed.), Frontier Country, Vol. 1 (Weldon Russell Publishing, Willoughby, 1989). [Ref.]
- Saravanapavananthan N. 1982. Penetrating wound of the aorta by a bull’s horn. Injury. 13: 412- 413. [Ref.]
- Pal DK, Bora V, Bisoi SC, et al. 2002. Urethrorectal fistula by Bull horn injury. J Indian Med Assoc. 100: 47. [Ref.]
- Rau JBV. 1982. Bull gore injuries in rural areas. Indian J Surgery. 44: 664-671. [Ref.]
- Shashirekha CA, Krishnaprasad K, Agarwal V. 2012. Evisceration of small bowel through femoral triangle following exsanguinating bull gore injury. Euroasian J Hepato-Gastroenterology. 2: 54-55. [Ref.]
- Dogan KH, Demirci S, Erkol Z, et al. 2008. Injuries and deaths occurring as a result of bull attack. Agromedicine. 13:191-196. [Ref.]
- Sekhon MS, Khatri HL, Grewal SS, et al. 1983. Bull horn injury. Indian J Surgery. 486-488.[Ref.]
- Shukla HS, Mittal DK, Naithani YP. 1977. Bull horn injury-a clinical study. Injury- The British Journal of Accident Surgery. 9: 164-167. [Ref.]
- Murali M, Kushwaha AS. 2015. A severe Scrotal and chest injury due to Bull horn: Two case reports managed at Primary health care hospital. SEAJCRR. 4: 1938-1946. [Ref.]
- Gajbhiye AS, Shamkuwar A, Bokade A. et al. 2016. Surgical management of bull horn injury. International Surgery Journal. 3: 41-45. [Ref.]
- Martinez RD, Villegas CC, Rivadulla-Serrano I, et al. 2007. A not obvious but devastating injury. Emergencias. 19: 347-349. [Ref.]
- Kade A. 2010. The brutal damage caused by bull goring. Environmental Graffity. [Ref.]
- Patel RN, Devgarha S, Mathur RM. 2016. A rare case of bull horn injury to chest wall; flail segment on chest wall without associated rib fractures. International Journal of Advances in Case Reports. 3: 41-44.[Ref.]
- Idikula J, Moses BV, Sadhu D, et al. 1991. Bull horn injuries. Surg Gynaecol obstet. 172: 220-222. [Ref.]
- Singh H, Mahant TS, Narula IM, et al. 1980. Cattle horn injuries. Aust NZ J. Surg. 50: 620-621. [Ref.]
- Rudloff U, Gonzalez V, Esleban CT. 2006. A 10 year experience of bullfight injuries. J of Trauma-injury, infection &Critical Care. 61: 970-974. [Ref.]
- Chambers O, Girand C, Gouffrant JM, et al. 2003. A detailed examination of injuries to the head and neck caused by bull fighting, and of their surgical treatment; the role of the cervico-facial surgeon. Rev Laryngol Otol Rhinol. 124: 221-228. [Ref.]
- Casani Martinez C, Morales Suarez- Varela M. 2000. Bull horn lesions in childhood. Pediatrics. 105: 685-686. [Ref.]
- Senthilkumar S, Madan M, Mahesh MS. 2014. Bull Gore injury- Its impact and surgical management. International Journal of Biomedical and Advance Research (IJBAR). 5: 279-281. [Ref.]
- Casey GM, Grant AM, Roerig DS, et al. 1997. Farm worker injuries associated with bull-New York State 1991-1996. AAOHN J. 45: 393-396. [Ref.]
- Criddle LM. 2001. Livestock trauma in central Texas: cowboys, ranchers, and dudes. J Emerg Nurs. 27: 132-140. [Ref.]
- Nod for tracking stray cattle with microchips. The Hindu, New Delhi: Online edition of India’s National Newspaper Wednesday, April 6, 2005. [Ref.]
- An appeal to end stray cattle menace in Indian cities or urban India by closing or removing all illegal or unlicensed dairies and cattle sheds. [Ref.]


















