
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Case ReportDOI Number : 10.36811/jcri.2022.110027Article Views : 76Article Downloads : 43
Recurrent cardiac hydatid cysts ruptured intraoperatively during anesthetic induction for open-heart surgery
Redha Lakehal*, Soumaya Bendjaballah, Rabah Daoud, Khaled Khacha, Baya Aziza and Abdelmalek Bouzid
Faculty of Medicine Constantine 03, Constantine, Algeria
*Corresponding Author: Redha Lakehal, Department of Heart Surgery, Ehs Dr Djaghri Mokhtar, Constantine, Algeria; Email: lakehal.redha@gmail.com
Article Information
Aritcle Type: Case Report
Citation: Redha Lakehal, Soumaya Bendjaballah, Rabah Daoud, et al. 2022. Recurrent cardiac hydatid cysts ruptured intraoperatively during anesthetic induction for open-heart surgery. J Case Rept Img. 4: 01-04.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2022; Redha Lakehal
Publication history:
Received date: 20 December, 2021Accepted date: 31 December, 2021
Published date: 03 January, 2022
Abstract
Introduction: Cardiac localization of hydatid disease is rare (<3%) even in endemic countries. Affection characterized by a long functional tolerance and a large clinical and paraclinical polymorphism. Serious cardiac hydatitosis because of the risk of rupture requiring urgent surgery. The diagnosis is based on serology and echocardiography. The aim of this work is to show one of the fatal complications of this condition which arose intraoperatively during anesthetic induction.
Methods: We report the observation of a 37-year-old woman operated on in 2010 for a cardiac hydatid cyst presenting a recurrence of cardiac hydatid disease with two left intraauricular cysts expressed by palpitations with dyspnea. Preoperatively: dyspnea stage II of the NYHA. Chest x-ray: CTI at 0.58. ECG: RSR. Echocardiography: Two largest left atrial cysts: 47/40 mm compress the origin of the right pulmonary vein, 2nd cyst of 36/28 mm. The existence of another small caliber lateral cyst. Positive hydatid serology. The patient developed an anaphylactic shock of unexplained cause, which required the assistive CPB facility. Intraoperative exploration: The two ruptured cysts in the left atrium with multiple left intraatrial daughter vesicles. Gesture: Removal of daughter vesicles with sterilization with hypertonic saline.
Results: The postoperative consequences were favorable despite a prolonged stay in intensive care following a picture of acute respiratory distress syndrome.
Conclusion: Intracardiac rupture is a very serious complication and can produce dramatic pictures with sudden death. It can be responsible for allergic reaction, systemic embolism, pulmonary embolism and systemic metastases.
Keywords: Hydatid Cyst; Heart; Relapsing; Rupture; Surgery; Anaphylactic Shock; Cardiopulmonary Bypass; Prevention
Introduction
Cardiac localization of hydatid disease is rare (<3%) even in endemic countries [1]. Affection characterized by a long functional tolerance and a large clinical and paraclinical polymorphism. Serious cardiac hydatitosis because of the risk of rupture requiring urgent surgery. The diagnosis is based on hydatid serology and echocardiography [2]. Computed tomography (CT) and magnetic resonance imaging (MRI) are the other diagnostic tools. The treatment of cardiac hydatid cysts is surgery [3-4]. The aim of this work is to show one of the fatal complications of this condition which arose intraoperatively during anesthetic induction for open-heart surgery of 02 recurrent hydatid cysts of the left atrium in a patient already operated on for cardiac hydatid cyst.
Case report
We report the observation of a 37-year-old woman operated on in 2010 for a cardiac hydatid cyst, living in an endemic area of hydatid disease presenting a recurrence of cardiac hydatid disease with two left intraauricular cysts discovered during a motivated echocardiography by palpitations with dyspnea on exertion.
Preoperatively
Functional class showed NYHA stage II dyspnea. Chest x-ray showed a CTI at 0.58 without distortion of the heart contours. ECG enrolled in regular sinus rhythm. Echocardiography showed two larger left intraauricular cysts: 47/40 mm compress the origin of the right pulmonary vein, 2nd cyst of 36/28 mm. The existence of another small caliber lateral cyst. (Figures 1,2) Hydatid serology was positive.
The patient went into anaphylactic shock of unexplained cause during the anesthetic induction which required the installation of emergency cardiopulmonary bypass assistance due to the ineffectiveness of the medical treatment (Epinephrine at optimal dose) the hypertonic saline serum sponges were placed into the pericardial cavity to prevent contamination. Intraoperative exploration showed the two ruptured cysts in the left atrium with multiple ruptured and unruptured vesicles with left intra atrial proligerous membrane. The procedure consisted of ablation of ruptured and unruptured daughter vesicles and of the proligerous membrane with sterilization by hypertonic saline at 30% of the atrium and the left ventricle (Figure 03).
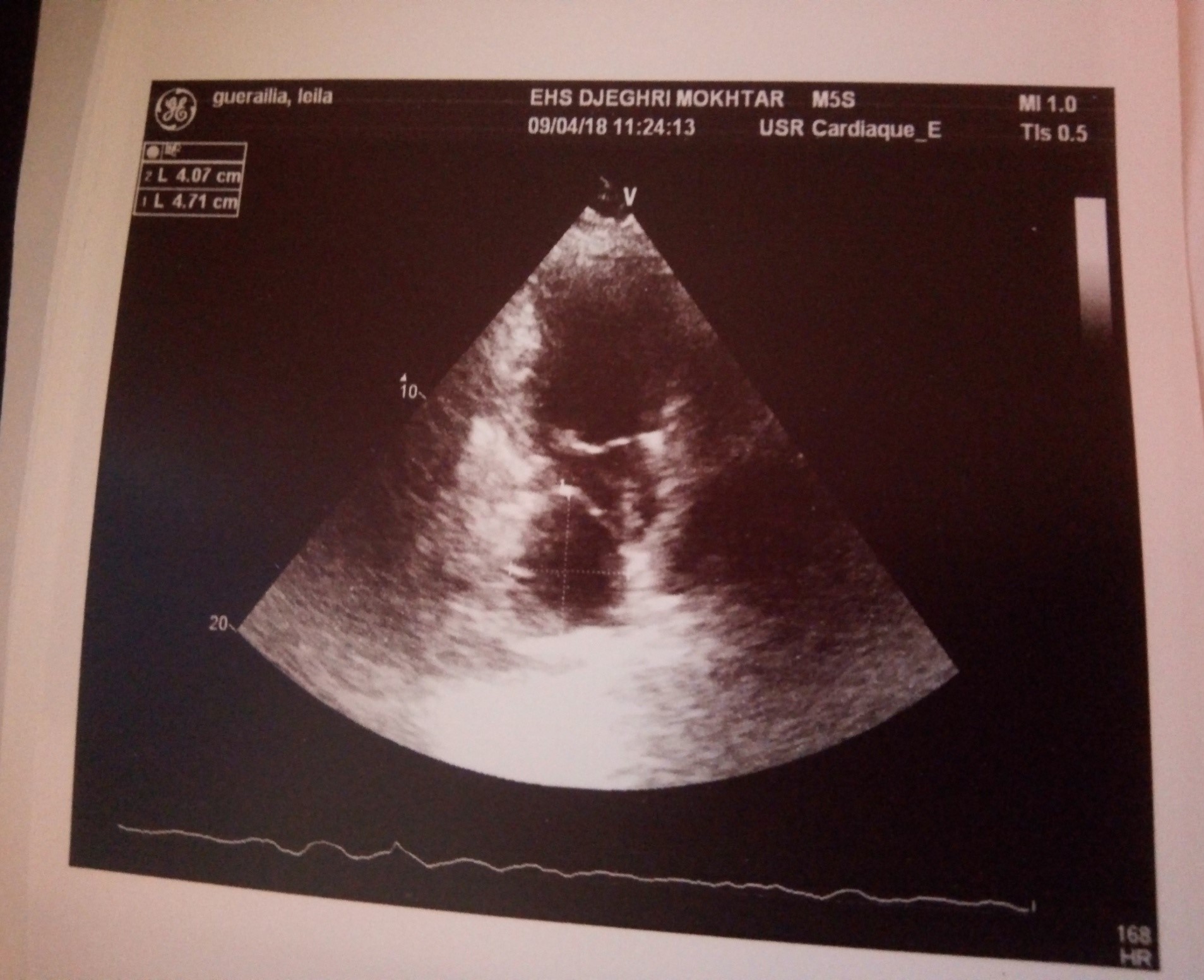
Figure 1: Echocardiographic image before rupture.

Figure 2: Echocardiographic image before rupture.

Figure 3: Intraoperative image
Extended intubation duration for 18 days linked to acute respiratory distress syndrome (ARDS) and associated pneumonitis. Stay in intensive care unit was 21 days. Length of postoperative stay was 15 days. The postoperative follow-up was relatively straightforward. She was put on Albendazol 02 tablet / day for one year with regular echocardiographic monitoring. The pathological study returned in favor of a cardiac hydatid cyst. The follow-up echocardiograms taken on the 1st, 3rd, 6th, 9th month and at one year did not show any cardiac recurrence.
Discussion
In the heart tissue, the disease involves approximately left ventricle with 46%, right ventricle with 21%, interventricular septum with 19.3%, right atrium with 9.7%, but pericardial, coronary sinus and left atrial involvement is very rare [5-6]. The recurrence of hydatid disease in this patient after several years is explained by a new re-infestation linked to the continued stay in an endemic area of hydatid disease. Intracardiac rupture of hydatid cysts of the heart is very frequent (38.66 %) and often causes sudden death (29 %) [7-9]. The consequences of the intracardiac rupture depend above all upon the contents of the cyst. If it contains liquid and microscopic elements, no mechanical disorders occur, but it may give rise to metastatic visceral echinococcosis. If it contains vesicles, or is degenerated, it may give rise to large emboli [7]. State of shock occurring on anesthetic induction was only explained during the opening of the left atrium and the discovery of the rupture of the two cysts during surgery in the full left atrium [10-11]. The table of acute respiratory distress syndrome developed by this patient during her stay in intensive care is explained by the state of anaphylactic shock; cardiopulmonary bypass and associated pneumonia [10-11]. The patient was put on medical treatment containing Albendazol for a year to prevent another recurrence of hydatid disease.
Conclusion
Intracardiac rupture is a very serious complication and can produce dramatic pictures with sudden death. It can be responsible for allergic reactions, systemic embolisms, pulmonary embolisms and systemic metastases. The real treatment for parasitic disease is echinococcosis control based on preventive measures that aim to interrupt the life cycle within hosts, health education and legislation.
References
1. Shehatha J, Alward M, Saxena P. 2009. Surgical management of cardiac hydatidosis. Tex Heart Inst J. 36: 72-73. Ref.: https://pubmed.ncbi.nlm.nih.gov/19436793/
2. Ipek G, Omeroglu SN, Goksedef D. 2011. Large cardiac hydatid cyst in the interventricular septum. Tex Heart Inst J. 38: 719-722. Ref.: https://pubmed.ncbi.nlm.nih.gov/22199447/
3. Orhan G, Ozay B, Tartan Z. 2008. Trente-neuf ans d’expérience Surgery of cardiac hydatid cysts. An experience of 39 years. 57. Ref.: https://pubmed.ncbi.nlm.nih.gov/17568556/
4. Funda Y, Bar?? T, Adnan TK. 2014. Cardiovascular Surgery and Interventions. 1: 3-5.
5. Birincioglu CL, Bardakci H, Kucuker SA. 1999. A clinical dilemma: cardiac and pericardiac echinococcosis. Ann Thorac Surg. 68: 1290-1294. Ref.: https://pubmed.ncbi.nlm.nih.gov/10543495/ DOI: https://doi.org/10.1016/s0003-4975(99)00692-x
6. Biyik I, Acar S, Ergene O. 2007. Left atrial mobile hydatid cyst mimicking left atrial myxoma and mitral stenosis and causing heart failure and arrhythmia. Int J Cardiovasc Imaging. 2: 193-195. Ref.: https://pubmed.ncbi.nlm.nih.gov/16868856/ DOI: https://doi.org/10.1007/s10554-006-9132-5
7. Raúl DB and Héctor M. 1963. Circulation. 27: 366-374.
8. Chadly AMD, Krimi SMD, Mghirbi TMD. 2004. Cardiac Hydatid Cyst Rupture as Cause of Death. The American Journal of Forensic Medicine and Pathology. 25: 262-264. Ref.: https://pubmed.ncbi.nlm.nih.gov/15322472/ DOI: https://doi.org/10.1097/01.paf.0000136443.46066.dc
9. Habib Thameur. 2001. World J Surg. 25: 58-67.
10. El Kouby A, Vaillant A, Comet B. 1990. L’hydatidose cardiaque: revue de la littérature récente à propos d’une expérience de quinze cas. Ann Chir. 44: 603.
11. Di Bello R, Mendez H. 1963. Intracardiac rupture of hydatid cyst of the heart: a study based on three personal observations and 101 cases in the world literature. Circulation. 27: 366. Ref.: https://pubmed.ncbi.nlm.nih.gov/14027496/ DOI: https://doi.org/10.1161/01.cir.27.3.366


















