
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Case ReportDOI Number : 10.36811/jcshd.2022.110023Article Views : 36Article Downloads : 20
Recurrent cardiac hydatid cyst located near the root of the superior vena cava and the interatrial septum: a case report
Redha Lakehal*, Farid Aymer, Soumaya Bendjaballah, Rabah Daoud, Khaled Khacha, Baya Aziza and Abdelmalek Bouzid
Faculty of Medicine Constantine 03, Constantine, Algeria
*Corresponding Author: Redha Lakehal, Department of Heart Surgery, Ehs Dr Djaghri Mokhtar, Constantine, Algeria; Email: lakehal.redha@gmail.com
Article Information
Aritcle Type: Case Report
Citation: Redha Lakehal, Farid Aymer, Soumaya Bendjaballah, et al. 2022. Recurrent cardiac hydatid cyst located near the root of the superior vena cava and the interatrial septum: a case report. J Cardiovasc Surg Heart Dis. 4: 01-04.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2022; Redha Lakehal
Publication history:
Received date: 20 December, 2021Accepted date: 30 December, 2021
Published date: 03 January, 2022
Abstract
Introduction: Cardiac localization of hydatid disease is rare (<3%) even in endemic countries. Affection characterized by a long functional tolerance and a large clinical and paraclinical polymorphism. Serious cardiac hydatitosis because of the risk of rupture requiring urgent surgery. The diagnosis is based on serology and echocardiography. The aim of this work is to show a case of recurrent cardiac hydatid cyst discovered incidentally during a facial paralysis assessment.
Methods: We report the observation of a 26-year-old woman operated on in 2012 for pericardial hydatid cyst presenting a cardiac hydatid cyst located near the abutment of the SCV discovered incidentally during an exploration for left facial paralysis: NYHA stage II dyspnea. Chest x-ray: CTI at 0.48. ECG: RSR. Echocardiography: Image of cystic appearance at the level of the abutment of the SVC. SAPP: 38 mmhg, EF: 65%. Thoracic scan: 30/27 mm cardiac hydatid cyst bulging the lateral wall of the right atrium and the trunk of the right pulmonary artery with fissured cardiac hydatid cyst of the apical segment of the right lung of the right lower lobe with multiple bilateral intra parenchymal and sub pleural nodules. The patient was operated on under CPB. Intraoperative exploration: Presence of a hard and whitish mass, about 03 / 03cm developed in the full right atrial wall opposite the entrance to the superior vena cava. Procedure: Resection of the mass removing the roof of the LA, the AIS and the wall of the RA with reconstruction of the roof of the RA by patch in Dacron and reconstruction of the IAS and the wall of the RA by a single patch in Dacron.
Results: The postoperative suites were simple.
Conclusion: The hydatid cyst is still a real endemic in Algeria, the cardiac location is rare but serious and can constitute a real surgical emergency, hence the importance of prevention.
Keywords: Hydatid cyst of the heart; Recurrence; Surgery; Cardiopulmonary Bypass; Prevention
Introduction
Hydatidosis is an anthropozoonosis caused by the development in humans of the larvae of Echinococcus granulosus. Cardiac localization of hydatid disease is rare (< 3 %) even in endemic countries [1]. Affection characterized by a long functional tolerance and a large clinical and paraclinical polymorphism [2]. Serious cardiac hydatitosis because of the risk of rupture requiring urgent surgery. The diagnosis is based on serology and echocardiography [2-3]. Computed tomography (CT) and magnetic resonance imaging (MRI) are the other diagnostic tools. The treatment of cardiac hydatid cysts is surgery [3-4]. The aim of this work is to show a case of recurrent cardiac hydatid cyst discovered incidentally during a work-up for facial paralysis.
Case report
We report the observation of a 26-year-old woman operated on in 2012 for pericardial hydatid cyst presented with a cardiac hydatid cyst located near the mouth of the superior vena cava (SVC) discovered incidentally during an exploration for left facial paralysis. Functionally, the patient had dyspnea stage II of NYHA. Chest x-ray showed a cardiothoracic index at 0.48. ECG enrolled in regular sinus rhythm. Echocardiography showed a cyst-like image at the mouth of the superior vena cava, SAPP: 38 mmhg and EF: 65%. Thoracic computed tomography (CT) showed a 30/27 mm cardiac hydatid cyst bulging the lateral wall of the right atrium and the trunk of the right pulmonary artery with fissured cardiac hydatid cyst of the apical segment of the right lung of the right lower lobe with multiple intra nodules. Bilateral parenchymal and sub pleural. Hydatid serology was positive. The patient was operated on under cardiopulmonary bypass. The hypertonic saline serum sponges were placed into the pericardial cavity to prevent contamination. Intraoperative exploration showed the presence of a hard and whitish mass, approximately 03/03 cm developed in the full right atrial wall opposite the entrance to the superior vena cava. (Figure 01).

Figure 1: The operation view.
The procedure consisted under cardiopulmonary bypass by resection of the mass carrying the roof of the left atrium (LA), the interatrial septum (IAS) and the wall of the right atrium (RA) (Figure 02) with reconstruction of the roof of the left atrium by patch of Dacron and reconstruction of the interatrial septum and the wall of the right atrium by a single patch of Dacron (Figure 03).
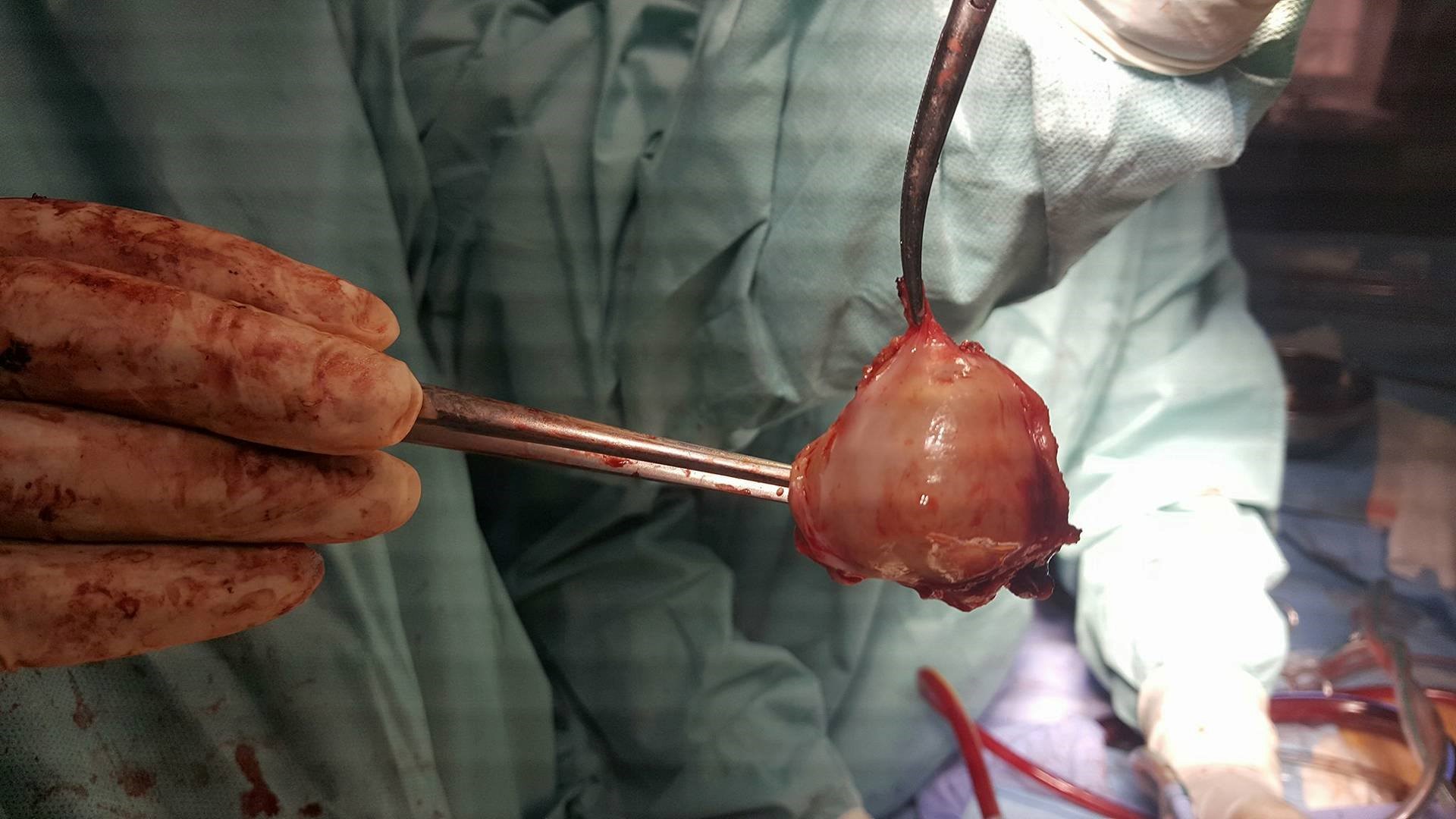
Figure 2: The operation view after complete resection of the hydatid cyst.

Figure 3: The operation view, reconstitution of the wall of the right atrium using a Dacron patch.
After the operation, there was no problem in the intensive care unit. The patient was discharged at the 10th postoperative day. The patient is still on Albendazol at the rate of 01 tablet / day for a year. The pathological study returned in favor of a cardiac hydatid cyst. The follow-up echocardiograms taken on the 1st, 3rd, 6th, 9th month and at one year did not show any cardiac recurrence.
Discussion
The right atrium is involved in only 3%-4% of cases [5]. In addition to the risk of rupture of the cardiac hydatid cyst, there is an added risk of obstruction of the opening of the superior vena cava resulting in superior vena cava [6]. Given the development of the cyst in the full wall of the roof of the left atrium; part of the interatrial septum and the wall of the right atrium, we had to resect the entire cyst with reconstruction of these structures with a Dacron patch [5]. It is important to remove the cyst without perforation to prevent dissemination and anaphylaxis [7], as is the case with our observation. In view of the recurrence of the cyst in a living patient in an endemic area of hydatid disease, the patient was placed on treatment with Albendazol tablets for one year with regular monitoring in order to prevent another recurrence [8-9].
Conclusion
The hydatid cyst is still a real endemic in Algeria. Cardiac localization is rare but serious. We reported this case to underline its atypical localization. It can constitute a real surgical emergency, hence the importance of prevention.
References
1. Shehatha J, Alward M, Saxena P. 2009. Surgical management of cardiac hydatidosis. Tex Heart Inst J. 36: 72-73. Ref.: https://pubmed.ncbi.nlm.nih.gov/19436793/
2. Ipek G, Omeroglu SN, Goksedef D. 2011. Large cardiac hydatid cyst in the interventricular septum. Tex Heart Inst J. 38: 719-722. Ref.: https://pubmed.ncbi.nlm.nih.gov/22199447/
3. Orhan G, Ozay B, Tartan Z. 2008. Trente-neuf ans d’expérience Surgery of cardiac hydatid cysts. An experience of 39 years. 57. Ref.: https://pubmed.ncbi.nlm.nih.gov/17568556/
4. Funda Y, Bar?? T, Adnan TK. 2014. Cardiovascular Surgery and Interventions. 1: 3-5.
5. Oraha AY, Faqe DA, Kadoura M. 2018. Cardiac Hydatid cysts; presentation and management. A case series. Ann Med Surg. 30: 18-21. Ref.: https://pubmed.ncbi.nlm.nih.gov/29946454/
6. Oner T, Korun O, Celebi A. 2019. A cardiac hydatid cyst mimicking a pericardial tumour in a paediatric case. Cardiol Young. 29: 244 246. Ref.: https://pubmed.ncbi.nlm.nih.gov/30511599/ DOI: https://doi.org/10.1017/s1047951118002032
7. Mansuroglu D, Omeroglu SN, Akdemir R. 2004. Right atrial hydatid cyst prolapsing into the tricuspid valve. Tex Heart Inst J. 31: 452-453. Ref.: https://pubmed.ncbi.nlm.nih.gov/15745306/
8. Bakkali A, Jaabari I, Bouhdadi H. 2017. Les kystes hydatiques cardiaques à propos de 17 cas opérés. Ann Cardiol Angéiol. 67: 67-73.
9. Bozbuga N, Erentug V, Akinci E. 2013. Is surgical therapy the only treatment of choice for cardiac echinococcosis with multiple organ involvement?. Interact Cardiovasc Thorac Surg. 2: 367-368. Ref.: https://pubmed.ncbi.nlm.nih.gov/17670072/ DOI: https://doi.org/10.1016/s1569-9293(03)00072-0


















