
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Case ReportDOI Number : 10.36811/ojor.2021.110013Article Views : 81Article Downloads : 44
Rhinolithiasis: A Rare Clinical Case
Sylvain Diembi1, Harol Boris Otouana2, Gerard Chidrel Gouoni2, A Tsieri Tsoba2, Brice Diabassana1, Franck Itiere Odzili2, Donatien Moukassa3, Gontran Ondzotto2
1Department of Otolaryngology, Adolphe SICE General Hospital, Pointe-Noire (Congo)
2Department of Otolaryngology, University Hospital Center, Brazzaville (Congo)
3Laboratory of Medical and Morphological Analysis, Edith Lucie BONGO ONDIMBA General Hospital (Congo)
*Corresponding Author: Dr. Sylvain Diembi, Department of Otolaryngology, Adolphe SICE General Hospital, Pointe-Noire (Congo), Pointe Noire, Tel: 00242055384152; Email: sdiembi@yahoo.fr
Article Information
Aritcle Type: Case Report
Citation: Sylvain Diembi, Harol Boris Otouana, Gerard Chidrel Gouoni, et al. 2021. Rhinolithiasis: A Rare Clinical Case. Open J Otolaryngol Rhinol. 3: 23-26.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2021; Sylvain Diembi
Publication history:
Received date: 20 September, 2021Accepted date: 28 September, 2021
Published date: 30 September, 2021
Abstract
Rhinolithiasis is a rare condition in our current practice. We report the case of a 19 year old woman, presenting with a double symptom marked by rhinorrhea and chronic unilateral nasal obstruction evolving since the age of 7 years, without any known foreign body. Rhinoscopy and nasal endoscopy coupled with CT scan were decisive examinations for the positive diagnosis. The therapeutic management consisted in the extraction of the rhinolithiasis resulting in the vacuity of the nasal cavity. The evolution was favorable with simple postoperative courses.
Keywords: Rhinolithiasis; Woman; Rhinoscopy; Endoscopic Surgery
Introduction
Rhinolithiasis is a rare or unrecognized condition and corresponds to a solid calcification by progressive deposition of calcareous salts around a central resorbable or non-resorbable foundation of normal shape and size [1]. Nasal endoscopy and imaging are essential for positive diagnosis. Described for the first time in 1654 by BARTHOLIN [1]. This rare pathology tends to disappear in Western countries, but remains relevant in underdeveloped countries due to poor socio-economic conditions, poor health coverage and the predominance of certain ethnocultural habits. The incidence of rhinolithiasis in underdeveloped countries is estimated at 3 new cases per year [1-3]. The absence of data on this pathology in the sub-region and in particular in our current practice justifies the publication of this clinical case.
Case report
Miss M. An, 19 years old, living in the city of Pointe-Noire, an industrial city (oil and wood exploitation) located in the south-west of the Republic of Congo - Brazzaville, without any particular pathological history, was received in outpatient clinic in March 2021 for purulent rhinorrhea, fetid, unilateral left, evolving since the age of 7 years. This recurrent rhinorrhea was frequently treated as rhinitis with episodes of irregular remission. It was associated with a nasal obstruction, homolateral, of progressive aggravation, intermittent headaches and two (2) months before the consultation, with a pain of the right hemiface. Nasal examination after aspiration of purulent secretions showed an irregular granulomatous tissue mass at the level of the right nasal vestibule, which was hard and stony on palpation with the stylet. This mass of grayish coloring, extending beyond the head of the inferior turbinate surrounded by an inflammatory granuloma. The CT scan showed a calcium density opacity centered by a hypodensity, which allowed the diagnosis of rhinolithiasis. The management consisted of an endoscopic extraction under general anesthesia, which led to a total vacuity of the right nasal cavity. The biochemical examination of the rhinolith found concretions made of mineral salts. The evolution was favorable at 3 months postoperatively.
Discussion
We described a case of rhinolithiasis in a 19 year old woman with no particular history, POLSON et al (2) and OZDEMIR et al (3) state that rhinolithiasis is present and frequent in women, often affecting young adults, but it can be observed at any age [2]. Pathogenically, rhinolithiasis can be of endogenous origin because the anatomical substratum consists of debris from cell lysis and desquamation associated with changes in the viscosity of nasal secretions potentiated by changes in the quality of the environment, i.e., pollution [1]. The city of Pointe-Noire is an industrial city where wood and oil are exploited, which may be an explanation. However, the exogenous origin is to be excluded since we did not find the notion of organic nasal foreign body or unrecognized or neglected in our patient [5,6,7]. The period of rhinolith formation varies from a few months to several years. Clinically, the dominant symptomatology is characterized by chronic unilateral purulent rhinorrhea and chronic nasal obstruction, associating anosmia and hemicrania in our patient, OZDEMIR et al [3] found rhinorrhea and nasal obstruction in 90% of cases in a study of 21 subjects. Other authors KHAROUBI, POLSON and NADIR [1,2,4] have described some symptoms such as epistaxis, headache, anosmia cacosmia and facial pain as described in our observation. NADIR et al [4] found asymptomatic rhinolithiasis which was discovered by chance on imaging (CT scan or standard radiography).
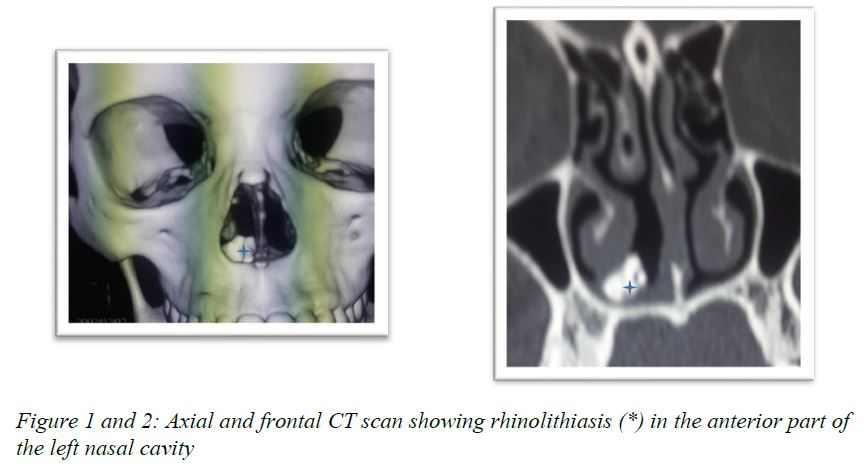
Rhinoscopy and nasal endoscopy allowed us to demonstrate an irregular granulomatous tissue mass in the right nasal vestibule, which was hard and stony on palpation with a stylet. This mass is grayish in color, extending beyond the head of the inferior turbinate and surrounded by an inflammatory granuloma. This description was found by some authors KHAROUBI, OZDEMIR [1,3], however NADIR et al [4] found a septal perforation associated with a synechia and a granuloma. The diagnosis is established on two clinical characteristics; the very hard or stony aspect and the sensation of crackling during exploration in button according to most authors [1,3,8,9]. It is on the basis of these arguments that we made the diagnosis in our study. The nose-sinus CT scan performed in our study revealed a calcium density opacity centered by a hypodensity. The diagnostic value of the CT scan has been accepted by many authors [1,3,9,10]. However, some authors have found metallic foreign bodies or an ectopic tooth [9,10]. The therapeutic choice in our study consisted in an endoscopic extraction with the use of rigid optics under general anesthesia, which resulted in a total vacuity of the right nasal cavity. Some authors [2,7-10] have preferred the external surgical approach of CADWELL-LUC, or lateral rhinotomy in case of giant rhinolithiasis, and finally lithotripsy, other authors have used local anesthesia for small rhinolithiasis [7]. After extraction, our surgical specimen was subjected to histo-biochemical analysis, a practice found in some authors [9,10]. In our study, the evolution was favorable, without complications, but recurrences of rhinolithiasis are exceptional [9,11] (Figure 1-3).

Conclusion
Rhinolithiasis is a rare condition in our country, affecting women, marked by a symptomatic duo rhinorrhea and chronic unilateral nasal obstruction, rhinoscopy and nasal endoscopy are decisive for the positive diagnosis, supported by the CT scan. Therapeutic management consists in the removal of the rhinolithiasis resulting in the vacuity of the nasal cavity.
References
1. Kharoubi S. 2007. Revue générale sur les rhinolithiases: à propos de 20 cas. J Tun Orl. 18: 34-39.
2. Polson CJ. 1943. On rhinoliths. J Laryngol Otol. 58: 79-116.
3. Ozdemir S, Akbas Y, Gorgulu O. 2010. Rhinolithiasis: Review of 21 cases. Am J Rhinol Allergy. 24: 136-139. Ref.: https://pubmed.ncbi.nlm.nih.gov/20977836/ DOI: https://doi.org/10.2500/ajra.2010.24.3553
4. Nadir Y, Atilla A, Murat S. 2008. Rhinolithiasis: Clinical Radiological and mineralogical factures. Am J Rhinol. 22. 78-82. Ref.: https://pubmed.ncbi.nlm.nih.gov/17976254/ DOI: https://doi.org/10.2500/ajr.2007.21.3112
5. Kharoubi S. 1998. Rhinolithiasis associated with septal perforation: a case report. Acta otorhinolarryngol Belg. 52: 241-245. Ref.: https://pubmed.ncbi.nlm.nih.gov/9810460/
6. Kanshik V, BhallaK, Pahade A. 2004. Rhinolithiasis. Ear Nose Thorat J. 83: 521-514. Ref.: https://pubmed.ncbi.nlm.nih.gov/15487624/
7. Aksungur EH, BinokayFB, Bicakcik. 1999. A Rhinolith which is mimicking a nasal benign tumor. Eur J Radiol. 31: 53-55. Ref.: https://pubmed.ncbi.nlm.nih.gov/10477099/ DOI: https://doi.org/10.1016/s0720-048x(98)00031-x
8. Mink A, Gati I, Szekely J. 1991. Nasolith removal with ultrasounnd lithotripsy. HNO. 39: 116-117. Ref.: https://pubmed.ncbi.nlm.nih.gov/2050554/
9. Vink, BW Van, Wormald R. 2008. A case of rhinolithiasis in Botsawana: A mineralogical, microscopic and cheminal study. J laryngol otol. 116: 1036-1040. Ref.: https://pubmed.ncbi.nlm.nih.gov/12537618/ DOI: https://doi.org/10.1258/002221502761698793
10. Elboukhani A, Touati M, Eljalil A. 1995. Rhinolithiase: A propos d’un cas et revue de la littérature. Lettre d’ORL et de chirurgie cervico-faciale. 201: 25-27.
11. Sacko HB. 1995. Rhinolithiase à propos d’une observation et revue de la littérature. Lettre d’Oto-Rhino-Laryngologie et chirurgie cervico-faciale. 201: 17-18.


















