
-
Mail us:
editor@raftpubs.org
- ISSN : 2583-1534
Indexing & Abstracting
Full Text
Case ReportDOI Number : 10.36811/ojrmi.2019.110003Article Views : 9Article Downloads : 14
Internal carotid artery injury secondary to acupuncture revealed using MRI
Yiu Ming WONG
Hong Kong Physically Handicapped & Able Bodied Association, Hong Kong
*Corresponding Author: Yiu Ming WONG, PhD, Hong Kong Physically Handicapped & Able Bodied Association, Health Science Unit (PEC), S102, G/F, Lai Lo House, Lai Kok Estate, Shamshuipo, Kowloon, Hong Kong, Tel: (852) 2351-7762; Fax: (552) 2958-1280; Email: pt@acupuncture-lab.org
Article Information
Aritcle Type: Case Report
Citation: Yiu Ming WONG. 2019. Internal carotid artery injury secondary to acupuncture revealed using MRI. O J Radio Med Img. 2: 23-27.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2019; Yiu Ming WONG
Publication history:
Received date: 12 November, 2019Accepted date: 15 November, 2019
Published date: 18 November, 2019
Abstract
A case of a lumbar spinal cord injury survivor, complained of gradual onset of left-arm weakness after simultaneous moxibustion and acupuncture treatment in which two moxibustion sticks were placed on his lower legs and eight acupuncture needles were inserted into his face and neck while he was in a sitting position. During the treatment, he had a forceful sneeze that his head leaned forward while his body remained upright. This momentary posture caused his right clavicle to press on the needle inserted at the right side of his neck, consequently, the accidental displacement of the needle dissected a portion of the right internal carotid artery as confirmed using MRI. Hospitalization and antiplatelet therapy were prescribed for his condition; he made a full recovery and was discharged in two days. Three months later, he received a Doppler ultrasound for the internal carotid artery that showed no abnormality.
Keywords: Acupuncture; Moxibustion; Adverse effect; Internal carotid artery
Introduction
Moxibustion and acupuncture are two methods in traditional Asian medicine that have been practiced in Asia for thousands of years. While the cultural belief in Asia is that the methods can cure a range of diseases, modern evidence suggests the modalities are effective merely for pain management [1]. In addition, the modalities are not risk-free. Moxibustion has been documented as being associated with local burns and respiratory allergic reaction [2,3]. Infection, pneumothorax and vascular injuries caused by acupuncture have been repeatedly reported [4,5]. The popliteal artery and vein are the most frequently affected vascular vessels [6], and in certain cases, the vascular injury was life-threatening [7]. In events on the posterior neck region, medulla and vertebral artery injuries have been reported [8,9]. A potential risk of the carotid artery being injured by acupuncture has been reported in literature [10], but actual cases are rarely seen. The present case illustrated an individual who suffered an internal carotid artery injury secondary to sneezing during simultaneous moxibustion and acupuncture treatments.
Case Report
A 48-year-old man with a 10-year complete L5 spinal cord injury visited our outpatient clinic; he was hemodynamically stable and alert. He complained of gradual onset of left-arm weakness after the simultaneous moxibustion and acupuncture treatment he had received 15 hours prior. This was also his first time receiving the traditional Asian medicine for his blurred vision related to macular degeneration. The treatments included: 2 adhesive moxibustion sticks placed on the skin of his fibular heads (bilateral acupoint GB34), 8 acupuncture needles with a shaft length of 4 cm inserted into the infraorbital region of his face (bilateral acupoints ST1-ST4) and 2 needles placed into his neck as an anterior margin of the middle sternocleidomastoid at the height of the laryngeal prominence (bilateral acupoints ST9) (Figure 1); the needle insertion depths were approximately 0.5 – 0.8 cm. The treatment duration was initially set for 15 minutes. Smoke released from the moxibustion sticks might have irritated the patient’s nasal mucosa; while sitting in his wheelchair, the patient had a forceful sneeze after five minutes. His head leaned forward while his body remained upright; this momentary posture caused the needle inserted at the right ST9 acupoint to press on the right clavicle, consequently displacing the needle posteriorly and superiorly (Figure 2). After the patient complained of sharp neck pain, his acupuncturist discontinued the treatment and removed all moxibustion sticks and acupuncture needles; the pain completely disappeared within one hour. A few hours later, the patient noted a bruising over his anterior right neck. Then his left-arm weakness slowly developed.
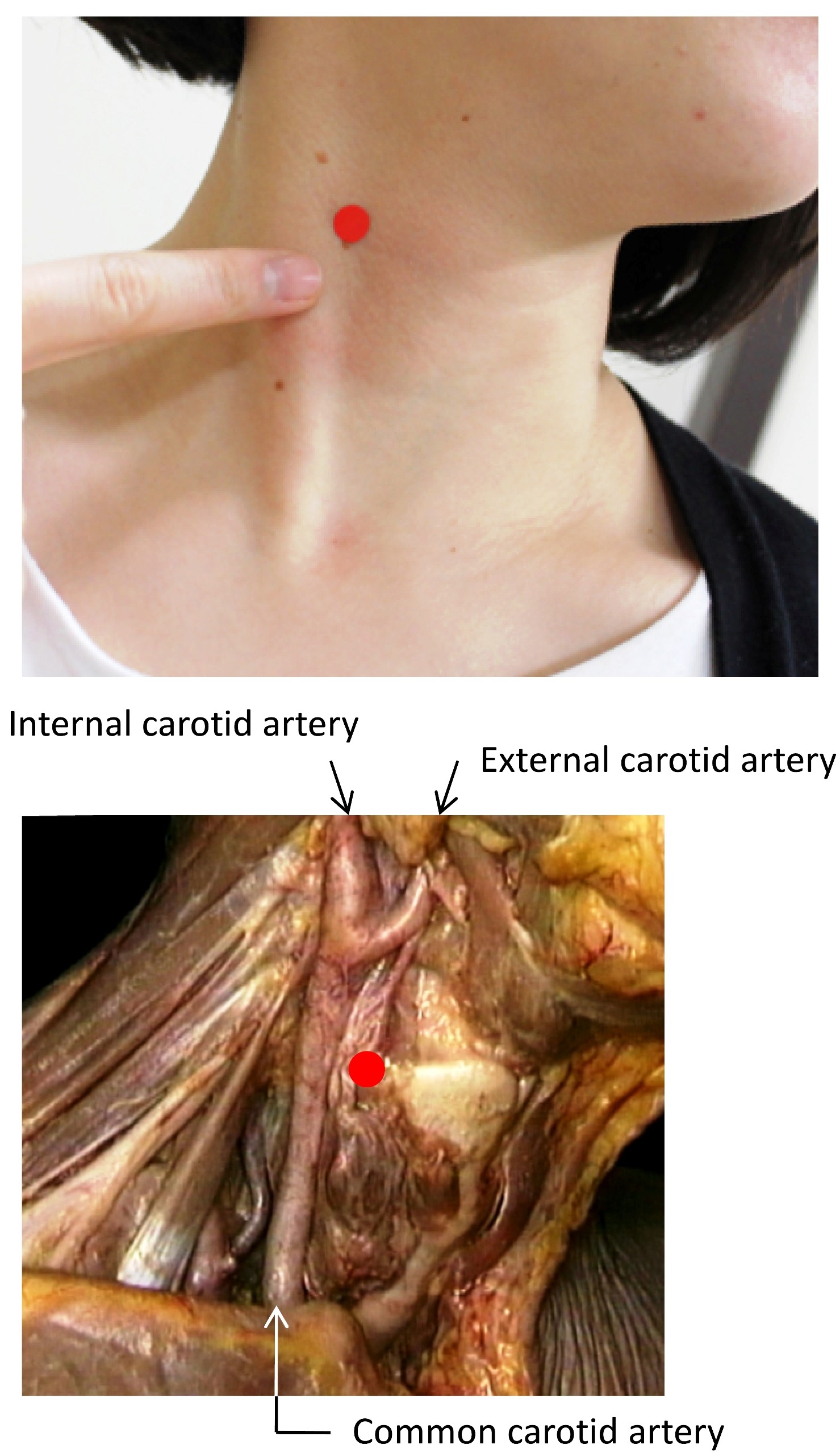
Figure 1: Acupoint named ST9 at the middle sternocleidomastoid for the right anterior neck; the corresponding anatomical specimen with skin and sternocleidomastoid muscle moved (photo courtesy of Wolters Kluwer).
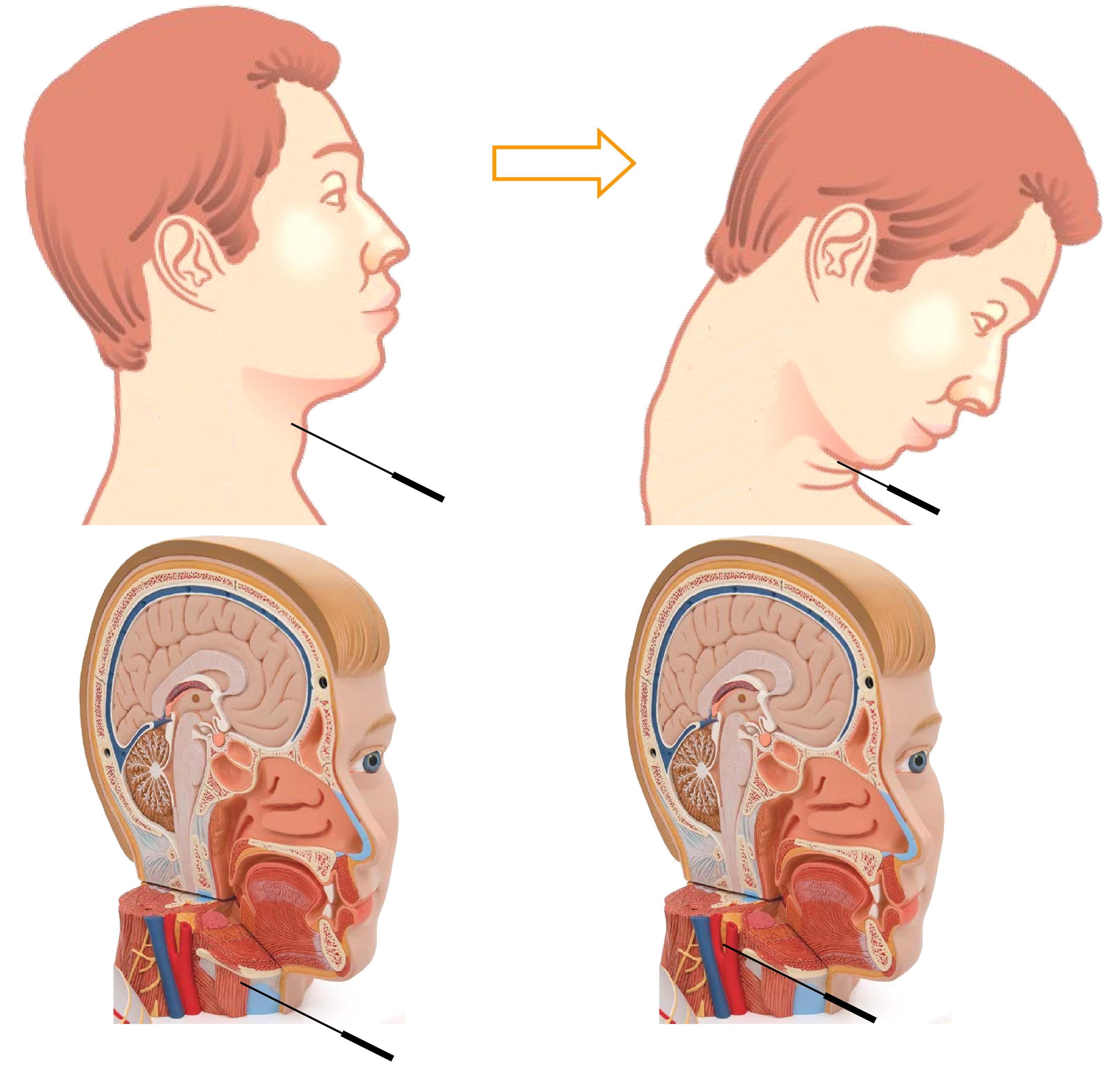
Figure 2: Accidental posterior-superior needle displacement as injury mechanism of the present case.
The patient had no medical conditions other than the above mentioned. In addition, his physical examination was unremarkable except the left arm weakness. Manual muscle strength testing for his left upper extremity graded that his shoulder flexion was 2, elbow flexion was 3, elbow extension was 2, wrist flexion was 3, wrist extension was 2, finger flexion was 3-and finger extension was 2-,while his right side counterparts were graded 5. The upper extremity sensation under the brush-light touch test was unremarkable and the biceps tendon reflex examination was graded normal bilaterally. Our key query was a hemorrhagic or ischemic stroke and an injury of the cervical vessels [11]. A cross-sectional T1-weighted MRI was performed on his brain and neck, and the only abnormality detected was the right internal carotid artery dissection at the C2 level; a tear developed in the intima of the artery with and formation of the false lumen that might have resulted from the displaced needle (Figures 2 and 3).
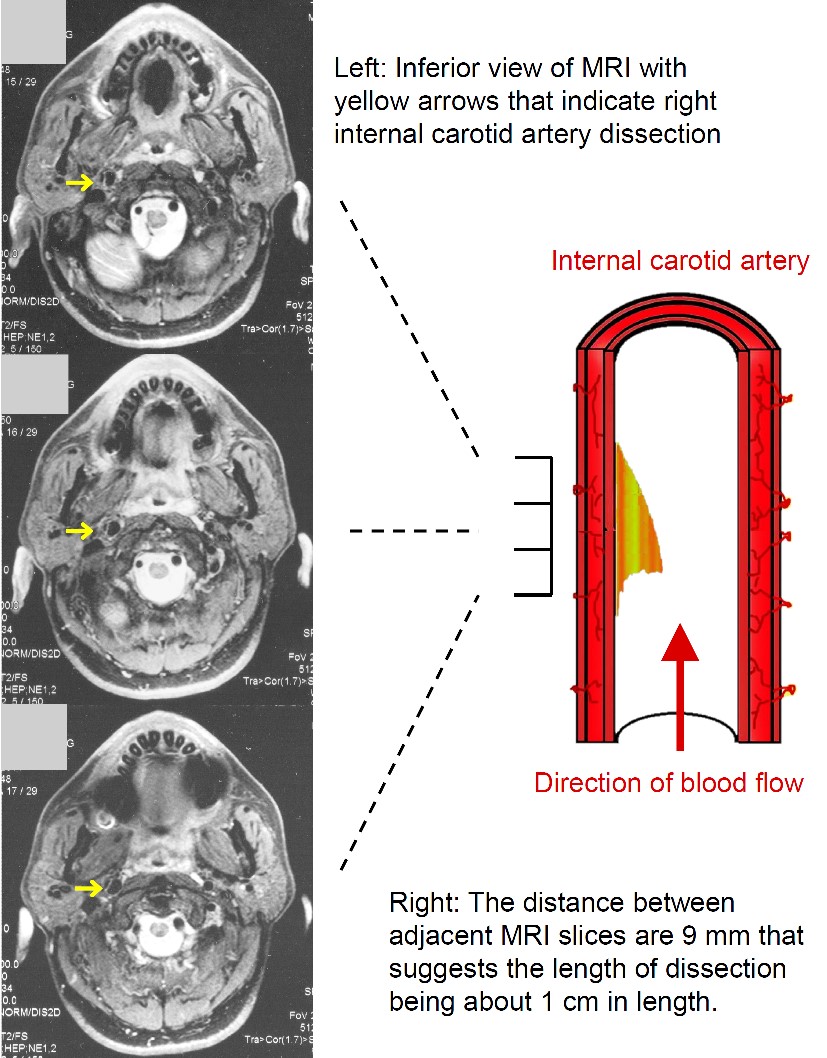
Figure 3: Cross-sectional MRI images showed an internal carotid artery dissection.
The treatment approach for the stable carotid artery dissection usually aims to prevent complications, while the artery may take about three to six months to heal [12]. In the present case, because the right internal carotid artery dissection may lead to the formation of a fibrin thrombus and result in potential ischemic stroke [11], the patient was requested to stay in a local hospital for observation and he was prescribed a daily 325mg-aspirin. After two-days inpatient care, his left-arm strength was fully regained and he was discharged with a daily dose of 81 mg-aspirin. On a post three-month follow-up, a Doppler ultrasound was performed for the internal carotid artery that showed no abnormality. His daily intake of aspirin was also ceased.
Discussion
In the present case, the patient with a spinal cord injury had received acupuncture and moxibustion for his blurred vision related to macular degeneration [13]; the outcome in this case was undesirable. The combination of the patient’s sneezing (forceful neck flexion movement) and two acupuncture needles being placed onto his anterior neck could be identified as a root cause of the accidental internal carotid artery injury. Relatively, people with a spinal cord injury have a higher sensitivity to airborne pollutants and a lower threshold of coughing and sneezing [14], thus the application of moxibustion for them may be precautious.
Ancient acupuncture needles were made of animal bone, copper, and iron, and were quite thick and rigid by modern standards. Thus, needle insertion was not deep for the sake of patient safety. Fine and flexible needles were initially developed by the Japanese in the 16thcentury using materials of gold and silver. Stainless-steel needles were not produced until after World War II and are commonly used by today’s acupuncturists worldwide [15]. The use of thin needles reduces the penetration discomfort and facilitates insertion depth, but they are prone to unintentional over-insertion and relevant internal organ injuries. Acupuncturists who underestimate the distance of the tip of acupuncture needles adjacent to vital structures, their ignorance of anatomical variance among individuals, and the use of improper needle lengths, likely contribute to the injuries of major blood vessels. If the acupuncture needle shaft was 1 cm or shorter in the present case, the consequent vascular injury might have been avoidable.
Conclusion
The present case demonstrates that a combination of neck acupuncture and sneezing caused an acupuncture needle displacement and traumatic injury to a carotid artery. Acupuncturists should not relax precautions when they apply neck acupuncture, since patients’ involuntary movement such as sneezing can lead to unpredictable consequences. The present case demonstrates that a combination of neck acupuncture and sneezing caused an acupuncture needle displacement and traumatic injury to a carotid artery. Acupuncturists should not relax precautions when they apply neck acupuncture, since patients’ involuntary movement such as sneezing can lead to unpredictable consequences.
References
1. Ramey DW. 2001. Acupuncture points and meridians do not exist. 5: 143-148. Ref.: https://bit.ly/2CH6z4t
2. Yamashita H, Tsukayama H, Tanno Y, et al. 1999. Adverse events in acupuncture and moxibustion treatment: a six-year survey at a national clinic in Japan. 5: 229-236. Ref.: https://bit.ly/379bU2a
3. Hsu YC, Chao HR, Shih SI. 2015. Human exposure to airborne aldehydes in Chinese medicine clinics during moxibustion therapy and its impact on risks to health. 50: 260-271. Ref.: https://bit.ly/355jFod
4. Bang MS, Lim SH. 2005. Paraplegia caused by spinal infection after acupuncture. 44: 258-259. Ref.: https://bit.ly/2piGBB2
5. Chauffe RJ, Duskin AL. 2006. Pneumothorax secondary to acupuncture therapy. 99: 1297-1299. Ref.: https://bit.ly/2KobWtE
6. Kuo HF, Shih MC, Kao WP, et al. 2010. Acupuncture-induced popliteal arteriovenous fistula successfully treated with percutaneous endovascular intervention. 26: 158-162. Ref.: https://bit.ly/2CH3UYu
7. Dang TN, Yeung AAC. 2016. Deep vein thrombosis and pulmonary embolism as a complication of traditional Chinese acupuncture and cupping. 10: 46-49. Ref.: https://bit.ly/2NP3NAw
8. Murata K, Nishio A, Nishikawa M, et al. 1990. Subarachnoid hemorrhage and spinal root injury caused by acupuncture needle - case report. 30: 956-959. Ref.: https://bit.ly/33SjXhS
9. Fukaya S, Kimura T, Sora S, et al. 2011. Medulla oblongata injury caused by an acupuncture needle; warning for serious complications due to a common method of alternative medicine. 258: 2093-2094. Ref.: https://bit.ly/2qVnsWa
10. Peuker E, Cummings M. 2003. Anatomy for the acupuncturist - facts & fiction 1: The head and neck region. 21: 2-8. Ref.: https://bit.ly/2Qkmbmr
11. Robertson JJ, Koyfman A. 2017. Extracranial cervical artery dissections. Emerg Med Clin North Am. 35: 727-741. Ref.: https://bit.ly/33VhxiQ
12. Rao AS, Makaroun MS, Marone LK, et al. 2011. Long-term outcomes of internal carotid artery dissection. 54: 370-375. Ref.: https://bit.ly/3706ir4
13. Neimtzow RC, Pham N, Burns SM, et al. 2006. Macular degenerative disease and acupuncture safety precautions. Med Acupunct. 17: 41-42.
14. Lin KH, Lai YL, Wu HD, et al. 1999. Cough threshold in people with spinal cord injuries. Phys Ther. 79: 1026-1031. Ref.: https://bit.ly/33PFl7E
15. Lao L. 1996. Acupuncture techniques and devices. J Altern Complement Med. 2: 23-25. Ref.: https://bit.ly/2Oj2Krk


















