
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Research ArticleDOI Number : 10.36811/ijfs.2019.110001Article Views : 491Article Downloads : 13
Female exposed to violence at Beni Suef governorate (Egypt) "2010-2014"
Sherien Salah Ghaleb1, Dalia Abd Elwhab Hassan2*, Amr Reda Zaki3 and Ahmed Jamal Sobhi Abdulla4
1Professor of Forensic Medicine and Clinical Toxicology Department, Cairo University, Egypt
2Lecturer of Forensic Medicine and Clinical Toxicology Department, Beni-Suif University, Egypt
3Assistant Professor of Forensic Medicine and Clinical Toxicology Department, Beni-Suif University, Egypt
4Assistant Lecturer of Forensic Medicine and Clinical Toxicology Department, Beni-Suif University, Egypt
*Corresponding author: Dalia Abd-Elwahab Hassan, Lecturer of Forensic Medicine and Clinical Toxicology Department, Beni-Suif University, Egypt, Tel: +2 01092373209; Email: daliaabdelwahab@ymail.com
Article Information
Aritcle Type: Research Article
Citation: Sherien Salah Ghaleb, Dalia Abd Elwhab Hassan, Amr Reda Zaki, et al. 2019. Female exposed to violence at Beni Suef governorate (Egypt) "2010-2014". Int J Forensic Sci. 1: 1-11.
Copyright:This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2019; Sherien Salah Ghaleb
Publication history:
Received date: 22 February, 2019Accepted date: 26 March, 2019
Published date: 28 March, 2019
Abstract:
Background: Violence has always been part of the human experience. Its impact can be seen, in various forms, in all parts of the world. Overall, violence is among the leading causes of death worldwide for people aged 15-44 years. “Gender-based violence (GBV) is the general term used to capture violence that occurs as a result of the normative role expectations associated with each gender, along with the unequal power relationships between the two genders, within the context of a specific society.” While women, girls, men and boys can be victims of GBV, the main focus of this resource package is on violence against women and girls.
Methodology: Data was retrieved from achieves of Beni Suef medico legal area from January 2010 to December 2014.
Aim of the work: The present study was done to demonstrate medico legal aspects of violence against females.
Conclusion: The study revealed that wives who faced violence were significantly young; exposure to violence indoors was less common than outdoors. Physical violence had several forms; the most common of which was blunt injuries followed by firearm, cut wounds, thermal, violent asphyxia, stabs, multiple (blunt+sharp), Neglicance and finally Carbamate toxicity.
Keywords: Violence against women and Egypt
Introduction
Women across the world, regardless of income, age or education, are subject to physical, sexual, psychological and economic violence. Experience of violence can lead to long term physical, mental and emotional health problems; in the most extreme cases, violence against women can lead to death [1]. The tireless work and effort of grassroots organizers, researchers, policy-makers and advocates over the past two decades have put violence against women and girls on the map as a critical issue to be addressed in the international arena. Donor organizations and international initiatives have dedicated funds and provide technical assistance for research and programmatic efforts aimed at preventing and responding to violence against women and girls [2]. Violence against women and girls causes pain, disability and death to an untold number of individuals every day, in every country in the world. Violence against women and girls was declared to be a violation of human rights by the United Nations (UN) General Assembly in 1993, in its Declaration on the Elimination of Violence Against Women. The UN Declaration defined violence against women and girls as including physical, sexual and psychological violence occurring in the family and general community, which is perpetrated or condoned by the State, and includes traditional practices such as child marriage and female genital cutting/mutilation (FGC/M). Violence against women and girls takes place in a multitude of contexts, including homes, schools, and the workplace [2]. The European Union defines ‘violence against women’ as "any act of gender-based violence that results in, or is likely to result in, physical, sexual or psychological harm or suffering to women, including threats of such acts, coercion or arbitrary deprivation of liberty, whether occurring in public or in private life"[3].
Egyptian wounded female
Through over 10 years of providing needy women with legal aid and consultation through our Legal Empowerment and Aid project, The Egyptian Center for Women's Rights has learned that women in Egypt are often subject to violence not only from family members and community members, but also by agents of the state, including the police supposedly tasked with the protection of all citizens. In addition, women are constantly subjected to violence in the form of sexual harassment and abuse on the street, and approximately ninety-seven percent of Egyptian women are the victims of female genital mutilation. Women’s right to lead a life free of violence is not widely internalized within Egyptian society, resulting in lack of reporting by victims of violence, lack of perpetrators’ awareness of the criminality of violence, lack of response from police and the legal system supposedly tasked with enforcing laws prohibiting violence, and perpetration of violence by authorities themselves against women in order to pressure their male relatives [4].
Female Genital Mutilation
Female Genital Mutilation in Egypt is reported to affect 90-97% of women. The practice ranges in severity from small cuts to the rarer complete removal of external genitalia followed by stitching of the vaginal opening. The origins of FGM in Egypt predate the arrival of both Christianity and Islam and are not part of the requirements of either religion. However, due to deeply ingrained cultural practices and its linkages to tradition, FGM has taken on religious dimensions in addition to its complex social function and association with purity, chastity and marriageability [4].The aim of this survey is to measure the evolution of violence against women as an important problem that facing the Egyptian community, which can be seen as the starting point for collecting information about the violence that women facing. The first important message that comes out of the study is the rising awareness of Egyptian community.
Subjects and Methods
Data of all female cases (total number of cases was 442), who were exposed to different types of violence which was gender based and have been reported to the medico-legal authority (registered in Beni Suef medico-legal area) from January 2010 to December 2014, were collected and analyzed after agreement from Beni Suef medico-legal area.
All data of these females were carefully saved and no names were mentioned for ethical consideration.
Exclusion criteria
Equivocal medico-legal reports, that did not confirm physical abuse, which needed more police investigations or there was suspicion of accidental injury.Some reports were not fully informative, i.e. absence of essential information related to perpetrators, victims and injuries or areas of victims’ origin and not sufficient data to exclude different predisposing factors which lead to violence against females. This was a descriptive retrospective study. For statistical purposes, cases were categorized according to the following parameters: -
• Age of victims ? divided into 8 groups, these are (1-10 yrs), (10- 20 yrs), (20-30 yrs), (30-40 yrs), (40-50 yrs), (50-60 yrs), (60-70 yrs) and (70-80 yrs).
• Residence of victims ? Urban, Rural.
• Relation of perpetrators to victims ? Intimate and stranger
• Gender of perpetrators ?male against female, female against female
• Place of violence exposure:
• Domestic violence ? inside home.
• Community violence ? outside home (rape and stalking).
• State violence ? exposure to state authorities (policemen).
• Type of violence:
• Physical violence ? blunt, sharp, firearm, thermal …. etc.
• Sexual violence or abuse ? rape, sexual harassment and alleged buggery by husband.
• Mixed (physical & sexual)
• Complications:
• No complications.
• Minor complications.
• Major complications.
• Disability. If alive
• Positive
• Negative
• End result of violence ? Fatal, non fatal (with or without complications).
Statistical Analysis
• Computer software package SPSS 15 was used in the analysis.
• Frequency and percentages were presented for quantitative variables.
• Chi-square and Fisher's Exact tests were used to estimate differences in qualitative variables. P value showed significance below 0.05.
Results
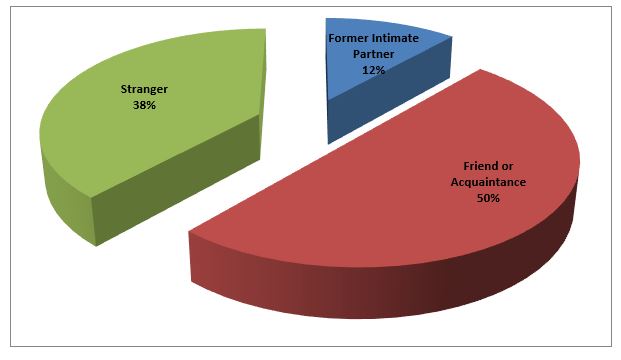
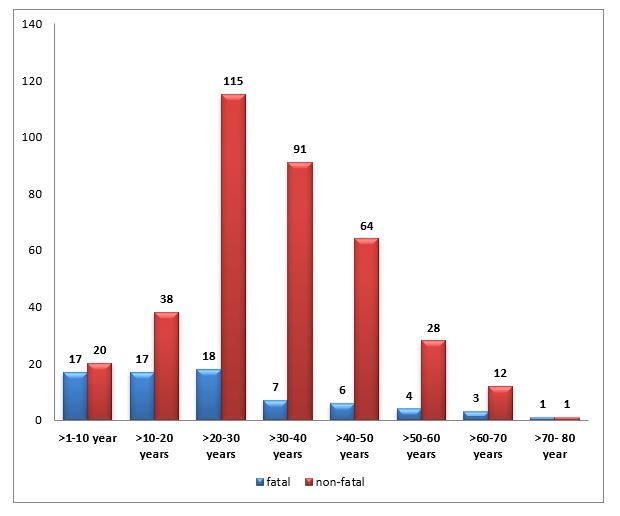
Regarding victim’s age, it was found that the majority were in the age group 20-30 years old (133 cases, 30.1%). It was noted that number of cases decreased with advancing of age as shown in figure 1. As regard the residence of the victim, 224 cases were living in rural comprising about 50.7% of the cases and 218 cases were living in Urban comprising about 49.3% of the cases. Physical violence (379 cases, 85.7%) had several forms, the most common of which was blunt injuries as shown in table 1. The current study showed that 7.9 % of the married females were pregnant during the assault. As for violence during pregnancy (35 cases, 7.9% of total cases), there is a unique complication for this type of violence which is abortion of the victim. Abortion happened in 2 cases (5.7% of cases of violence during pregnancy). Despite the scarcity of data, it is apparent that violence during pregnancy does contribute to miscarriage. Sexual assault is another form of violence against females (63 cases, 31.6%) as shown in table 2, figure 2. There are three types which are rape, sexual harassment and buggery by the husband. Total numbers of cases examined for rape was 26 cases, Twenty six cases (100% of alleged rape cases) had positive signs of rape, 2 of which (7.7% of causes of mortality) ended with death and 24 cases (92.3%) ended without as shown in table (3).In the current study, the perpetrator of the rape assault was a former spouse in 11.5% of cases, a friend or an acquaintance in 50% and a stranger in 38.5% as shown in figure 3. As regard the complications of sexual abuse, there were no records for complications of cases of rape examined at Beni Suef medico-legal area (50 cases). Five cases were complicated by vaginal and /or anal laceration, three cases were complicated by pregnancy, and three cases complicated by become prostitute. Cases of violence that had a fatal outcome showed (73 cases, 16.5%). Although the greatest number of cases was in the age group from 20-30 years (18cases, 23.3% of total mortality), the incidence of mortality in this age group was only 13.5% of cases. Fatality rate increased with the extremely of age as shown in figure 4. The remaining 1 case in the age group 70-80 was severely complicated with disability and disfigurement. Concerning the relation between injury type and prognosis of cases, it was found that although the firearm injuries were the most common type that had a fatal outcome (17 cases, 23.3% of mortality), this number represented 13.4% of total cases exposed to firearm injuries. As for blunt injuries (161 cases), 14 (19.2% of deaths) ended with mortality. Violent asphyxia (11 cases, 15.1% of mortality) all cases ended with death, this number represented 100% of cases exposed to violent asphyxia. Stabs (10 cases, 13.7% of mortality) all cases ended with death, this number represented 100% of cases exposed to stab wounds. So, stab wounds& violent asphyxia were more dangerous for causing death than other injuries. Neglicance (8 cases, 11 % of mortality) all cases ended with death, this number represented 100% of cases exposed to Neglicance. Burn was present in 18 cases, 5 (6.9% of deaths) ended with mortality. Carbamate toxicity (5 cases, 6.8 % of mortality) all cases ended with death, this number represented 100% of cases exposed to Carbamate toxicity.
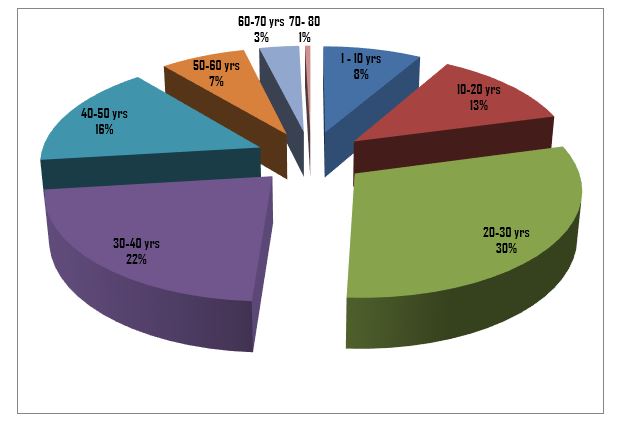
Figure 2: Distribution of different types of sexual violence.
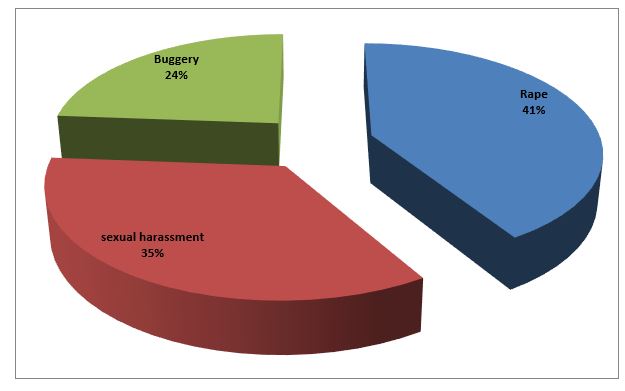
Figure 3: Relation between victim of rape and perpetrator.
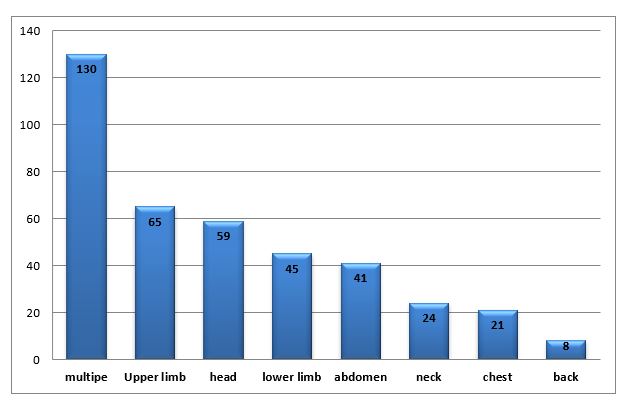
Rape homicide was recorded in 2 cases (2.7%), the cause of which was heavy blunt object. Other types of injuries (cut wounds, multiple (blunt+sharp)) were not complicated with mortality. The leading cause of death is firearm injuries, followed by violent asphyxia, followed by blunt injuries and lastly comes stab wounds. As regards site of injury, multiple site injuries were the most frequent (130 cases, 29.4% of total cases) as shown in figure 5. Regarding complications of physical violence, the most frequent complication was mortality (73 cases). This severe complication should draw attention for all measures to prevent violence against females. Then, comes in the 2nd order of complications the disability (66 cases) resulted from skeletal fractures, followed by disfigurement by acid throwing and sharp object (17 cases). Eye loss in (12 cases) caused by blunt injury was present in the 4th order. Skull fracture & P.C (9 cases) comes in 5th place in the sequence of complications. Injury of internal organs (like liver and spleen) was present in the 6th order (8 cases). Two cases of abortion complicate cases of violence during pregnancy (5.7% of this type of injury). Only cases with fatal outcome were studied for motivation as there was shortage of information in the archives of cases that ended with non-fatal outcome (Beni Suef medico-legal area). Regarding gender of perpetrator, the study results showed that male violence against female occur in majority of cases (400 cases, 90.5%), But there is female violence against female showed in (42 cases, 9.5 %).
Discussion
In the majority of countries, less than 40 per cent of the women who experience violence seek help of any sort, and among those who do, most look to family and friends as opposed to the police and health services. The percentage of women who seek help from the police, out of all women seeking help, is less than 10 per cent in almost all countries with data [1]. Women who reported being abused at least once in their lifetime were also more likely to experience a range of poor physical and mental health outcomes than those who had never been abused. Sexual, psychological and emotional violence inflicted by an intimate partner is also widespread. It is estimated that at least one in three women are subjected to some type of intimate partner violence" IPV" over their lifetime [2]. The present study revealed that wives who faced violence were significantly young, that means that as her age increases, the lesser that she experiences violence. This result was consistent to that reported by Kandeel et al., 20035. The cycle of violence begins between the ages of 15-49 [6]. According to U.S. Preventive Services Task Force (2004) [7], Women aged 16-24 years are more likely than other women to be victims of violence at the hands of an intimate.There are other studies on Egyptian society reported that 40% of women between the ages of 15 and 19and 20% of women 40 to 49 years old reported being beaten during pregnancy [8]. Fisher et al., (2003) [9] found that abused pregnant women were more likely to be hospitalized before delivery, suffer from premature labor, and deliver by Cesarean section. Rachana et al., (2008) [10] additionally found higher risk of abruption-placenta and preterm birth among abused pregnant women than among their non abused counterparts. In the current study, the perpetrator of the rape assault was a former spouse in 11.5% of cases, a friend or an acquaintance in 50% and a stranger in 38.5% as shown in figure 3. These results are in contrary with the false misconception that rape is committed mostly by strangers. Other survey done by US Bureau of Justice Statistics showed that the perpetrator was a current or formal intimate partner in 26% of cases), a relative in 7%, a friend or acquaintance in 38% and a stranger in 26% [11]. Australian government statistics showed that perpetrator was a current or formal intimate partner in 56% of cases, a relative in 10 %, a friend or acquaintance in 27% and a stranger in 8%. These statistics prove that most cases of rape are done by persons known to the victim not by strangers [12].
Intimate partner violence accounts for the majority of women’s experiences of violence. Prevalence of sexual violence is lower than that of physical violence; however, in intimate relationships they are often experienced together. Worldwide, 35 per cent of women have experienced physical and/or sexual violence by an intimate partner or sexual violence by a non-partner at some point in their lives. Two thirds of victims of intimate partner/family related homicides are women, while women represent only 20 percent of victims of all cases of homicides [1]. Acceptance of wife beating is generally higher in Africa, Asia and Oceania and lower in Latin America and the Caribbean and developed countries. However, attitudes towards violence are starting to change-in almost all countries where information for more than one year is available, the level of both women’s and men’s acceptance of violence has decreased over time. In most countries, levels of acceptance are lower among men than women [1].The most common type of physical violence was blunt injuries as shown in table 1, these results partial agree with studies at Monoufia University Hospital which shows that the most common injurious agent was blunt instrument (87.5%) followed by sharp instrument, thermal or chemical represented by 9.8% and 1.5% respectively, the least was firearm weapons and poisons represented by 0.6% for each [13]. Another study showed that the most common form was beating (71%), followed by burning (21%) finally stabbing (8%) [6].
| Table 1: Distribution of different types of Injuries in cases exposed to physical Violence. | ||
|---|---|---|
| TYPE | FREQUENCY | PERCENT (%) |
| • Blunt | 161 | 42.5 |
| • Cut | 29 | 7.7 |
| • Stab | 10 | 2.6 |
| • Firearm | 127 | 33.5 |
| • Burn | Inflammable liquid (e.g. kerosene) | 11 | 2.9 |
| • Burn | Corrosive burn (Acid throwing) | 7 | 1.9 |
| • Burn | • TOTAL | 18 | 4.8 |
| Multiple ( blunt+ sharp ) | 10 | 2.6 |
| Violent asphyxia | 11 | 2.9 |
| Carbamate toxicity | 5 | 1.3 |
| Neglect | 8 | 2.1 |
| TOTAL | 379 | 100 |
| Table 2: Distribution of Different Types of Sexual Violence. | ||||
|---|---|---|---|---|
| Type | Frequency | P value | ||
| Sexual | Sexual &Physical | Total | ||
| ? Rape | 13 | 13 | 26 | 0.151 |
| ? Sexual harassment | 12 | 10 | 22 | |
| ? Buggery | 12 | 3 | 15 | |
| TOTAL | 36 | 25 | 63 | |
| P value > 0.05= non significant P value <0.05= significant | ||||
| Table 3: Distribution of Cases of Rape | ||||
|---|---|---|---|---|
| Total number | 26 | |||
| Lived cases | 24(92.3 %) | |||
| Cases ended with death | 2 (7.7%) | |||
| P value > 0.05= non significant P value <0.05= significant | ||||
Cases of violence that had a fatal outcome showed (73 cases, 16.5%). These results disagree with studies in North America which shows that the incidence of mortality was about 40–60% from total cases [14]. Although the greatest number of cases was in the age group from 20-30 years (18cases, 23.3% of total mortality), the incidence of mortality in this age group was only 13.5% of cases in this age group. Fatality rate increased with the extremely of age as shown in figure 4. The remaining 1 case in the age group 70-80 was severely complicated with disability and disfigurement. This result could be explained by studies done on risk factors and vulnerability of elder persons done by Fulmer et al. (2004) [15], which show that old persons seem to be at greater risk than others. The characteristics that appear to make older adults most vulnerable are those which reduce their functional capacity or spawn problem behaviors. Sometimes these two types of characteristics are related. Reduced functional capacity can result from frailty, poor health, physical or mental impairment, or disability. Its effects may leave older adults unable to fend off or escape from elder abuse, and in some instances may even render them unable to recognize the seriousness of the problem. In addition, reduced functional capacity can render older adults dependent for care on others who are ill-equipped to provide it or resentful about having to do so. Finally, reduced functional capacity can limit an elderly person’s ability to seek help. For instance, mental illness may make them suspicious of outside assistance, sensory loss may inhibit use of telephones or other communication devices to signal need, and cognitive impairment may limit the ability of older adults to problem-solve and thereby identify sources of help and make contact with them [15].
According to research, areas of head, neck, and face (HNF) are the most commonly reported sites of injury, ranging in frequency from 50-80% [16]. Specifically, the middle third of the face has been found to be the most at risk [17]. This is followed by upper extremity injuries, which is consistent with the likelihood of receiving defense injuries. The least common sites of injury are to the abdomen and back [18]. Other Egyptian studies as the study conducted by (Abdel Salam, 2005) [19] on family violence cases in greater Cairo governorates over 6 years who found that death occurred in 56% of cases, permanent infirmity constituting 18.5% and complete recovery in only 25.5% of cases. Regarding gender of perpetrator, the study results showed that male violence against female occur in majority of cases (400 cases, 90.5%), But there is female violence against female showed in (42 cases, 9.5 %). The idea of women being violent is a hard thing for many people to believe, it goes against the stereotype of the passive and helpless female. These results agree with studies at Monoufia University Hospital which shows that the 89.2% of the assailants were males and 10.8% were females [13]. Another study showed that 76.8% of the assailants were males and 32.2% were females [19].
Researchers have estimated the incidence of pregnancy among rape victims of reproductive age to be significant, about 3-5% [20]. the survey done for pattern of intimate partner homicide in Michigan, USA agree with the results of our study, where firearm injuries were the leading cause of death (53%) followed by assault with sharp object (21%), then assault with violent asphyxia (7%) and assault with blunt object (7%), the remaining cases was unidentified cause of death [21]. Another study done in Australia agree with the results of the current study as follows, gun shots were the most common cause of death in homicides between sexual intimates (36%), followed closely by stabs (31%) which were frequently multiple in nature with over fifty cuts or lacerations inflicted. Violent asphyxia was the cause of death in 12% of cases, blunt injuries in 5% and thermal injuries in 3% of cases [22]. Other results are viewed in research of complications of violence against women done by Tjaden and Thoennes, (2000) [14] which shows that incidence of mortality due to violence against women is between 40-60% of total cases. The limitation for such analysis in this study was that the files of the archive were not properly recorded for such item. This finding was in agreement with the results of other studies carried by (El Zanaty and Way, 2006) [8] in Cairo and that carried out by (Gareeb, 2006) [23] in Assuit which concluded high incidence of family violence in rural areas.
Conclusion
Availability of data on violence against women has increased significantly in recent years-since 1995 [1]. This study was conducted to evaluate the forensic aspects of the phenomenon of the violence against females from data retrieved from achieves of cases admitted to Beni Suef medico-legal area from January 2010 to December 2014. The perpetrators were commonly found to be intimate partner to the victim and mostly known persons to the victim and/or family rather than to be unknown to the victim. It was obvious that perpetrator of rape was known to the victim rather than to be stranger. Regarding gender of perpetrator, were commonly found that male violence against female occur in majority of cases, but there is female violence against female. In Egypt, a husband who forces his wife to have sexual intercourse is not considered by law to have committed a criminal offence since woman is legally obliged, due to marriage contract, to obey her husband and to follow him to bed each time he asks her, and she can only refuse for a legally valid reason which I consider it to be the most harmful violence against women. There is a difficulty in determining the number of sexual assaults which is under-reporting. Guilt, fear of retribution, humiliation, lack of knowledge of and trust in the legal and medical system, and impaired cognitive processing that occurs following intense trauma are some reasons why females may not report.
Recommendations
Violence is preventable. Evidences showed strong relationships between levels of violence and potentially modifiable factors such as poverty, income and gender inequality, use of alcohol, and the absence of safe, stable, and nurturing relationships between female children and parents. Changing cultural and social norms that support violence is a must. Care and support programs should be designed to face the consequences of violence against female. Strengthening of religious morals and kinship that recommend respect of elders and care of female should be done.
References
- http://unstats.un.org/unsd/gender/worldswomen.html
- Shelah s. Bloom. violence against women and girls; a compendium of monitoring and evaluation indicators, USAID EAST AFFRICA. 2008. [Ref.]
- http://www.consilium.europa.eu/uedocs/cmsupload/16173cor.en08.pdf
- The Egyptian Center for Women's Rights: www.ecwregypt.org, www.fourliteracies.org and www.awfarab.org
- Kandeel H, Toama Z, Sobhy S, et al. 2003. Identifying the patterns and factors contributing to domestic violence against pregnant women. ASNJ, 2.[Ref.]
- Abdel Wahhab L. 1994. Domestic violence in Egypt, Dar Elmada Lilthaqafa Walnashr, Birut, Lebanon.[Ref.]
- US Preventive Services Task Force 2004. Screening for family and intimate partner violence: Recommendation statement. Annual Family Medicine. 2: 156-160. [Ref.]
- El Zanaty F, Way A. 2000. "Egypt demographic and health survey2005. Cairo, Egypt: National Population Council, Ministry of Health& Population, El Zanaty Association & Macro International". 17: 222-230. [Ref.]
- Fisher M, Borochowitz Y, Neter E. 2003. "Domestic abuse in pregnancy: Results from a phone survey in Northern Israel". 5: 35-39. [Ref.]
- Rachana C, Suraiya K, Hirsham A, et al. 2008. "Prevalence and complications of physical violence during pregnancy". European Journal of Obstetrics and Gynecology and Reproductive Biology.103: 26-29. [Ref.]
- US Bureau of Justice Statistics 1999. Compendium of Federal Justice Statistics. [Ref.]
- Australian Bureau of Statistics 2004. Sexual Assault in Australia: A Statistical Overview.[Ref.]
- Badawy. 2014. A prospective study of some medicolegal aspects of physical and sexual family violence cases at Menoufia University hospital over 2 years. [Ref.]
- Tjaden P, Thoennes N. 2000. Full report of the prevalence, incidence, and consequences of violence against women: Findings from the National Violence against Women Survey. Washington, DC, National Institute of Justice, Office of Justice Programs, US Department of Justice and Centers for Disease Control and Prevention (NCJ 183781). [Ref.]
- Fulmer T, Dong X, Simon M, et al. 2004. Elder self-neglect and abuse and mortality risk in a community-dwelling population. Journal of the American Medical Association. 302: 517-526. [Ref.]
- Biroscak B.J, Smith P.K, Roznowski H, et al. 2006. intimate partner violence against women: Findings from one state’s ED surveillance system. 32: 12-16. [Ref.]
- Le B.T, Dierks E.J, Ueeck-Homer L.D, et al. 2001. Maxillofacial injuries associated with domestic violence. Journal of Oral and Maxillofacial Surgery. 59: 1277-1283. [Ref.]
- Brismar B, Bergman B, Larsson G, et al. 1987. Battered women: Adiagnostic and therapeutical dilemma. Acta Chirurgica Scandinavica, 153: 1-5. [Ref.]
- Abdel Salam Y. 2005. "study on Family violence: Partner and Child Abuse cases reported to the greater Cairo Department and Morgue from January 1998 to December 2003."Master Thesis, Faculty of Medicine, Zagazig University.[Ref.]
- Masho S.W, Odor R.K, Adera T. 2005. Sexual assault in Virginia: A population-based study. Women’s Health Issues. 15: 157-166. [Ref.]
- Brian J, Patricia K. 2005. Intimate partner homicide in Michigan 1999-2003.[Ref.]
- Easteal P. 1991. Homicide between sexual Intimates in Australia: A preliminary report. [Ref.]
- Gareeb A. 2006. "Study of domestic violence among attendants of outpatient clinics in Assuit university hospital". Doctorate Thesis, Faculty of Nursing, Assuit University.[Ref.]


















